Doughnuts on a production line inside a Krispy Kreme Doughnuts store in Times Square in Manhattan.
Angus Mordant/Bloomberg
Krispy Kreme
is leading a group of six companies to the public markets on Thursday.
Besides the doughnut chain,
Acumen Pharmaceuticals,
D-MARKET Electronic Services & Trading,
Evercommerce,
Torrid Holdings,
and the
Glimpse Group
opened for trading.
So far this week, 17 companies, including the current six, have listed their shares. There are no initial public offerings on tap for Friday because of the holiday weekend. On Wednesday, 10 companies went public, with
Didi Global,
the Uber of China, trading flat and closing at $14.14, 14 cents above its offering price.
On Thursday, Acumen Pharmaceuticals (ticker: ABOS) was one of the first to begin trading. The stock opened at $25.07, hit a high of $26.98, and recently changed hands in afternoon trading at $20.98, up 31% from the offering price.
The solid performance came after Acumen increased the size of its deal by nearly 20%. The biotech company, which is developing therapies to treat Alzheimer’s disease, collected about $160 million. It sold roughly 10 million shares at $16, the top of its $14-to-$16 range.
The Glimpse Group (VRAR), which develops and commercializes virtual and augmented reality software products, also opened. Shares kicked off at $11.75, peaked at $16.44, and recently traded at $12.95, up nearly 85%. Glimpse delivered Thursday’s smallest deal. The company collected $12.3 million, after selling 1.75 million shares at $7, the midpoint of its $6-to-$8 price range.
Torrid Holdings (CURV) began trading, with shares rising 15% from its offering price to $24.18 in afternoon trading. The plus-size, direct-to-consumer women’s retailer increased the size of its deal twice. It filed to offer 8 million shares at $18 to $21, which it boosted Wednesday to 10 million. It ended up selling 11 million shares at $21, the top of its expected range, raising $231 million. Sycamore Partners, the retail-focused private-equity firm, will own nearly 76% of Torrid after the IPO.
Krispy Kreme (DNUT), the most well-known of Thursday’s group, kicked off at $16.30, peaked at $20.17 and recently changed hands at $19.57, up 15% from the offer price. The doughnut chain increased the size of its deal by 10% but priced well below its expected range to raise $500 million. Krispy Kreme had planned to offer 26.7 million shares at $21 to $24 each, but ended up selling 29.4 million shares at $17 each. JAB Holding, the European investment firm, will own about 39% of Krispy Kreme after the IPO
D-Market Electronic Services & Trading, or Hepsiburada (HEPS), jumped 8% from its offer price and is trading at $13. Hepsiburada, which means “you can find anything you want here” in Turkish, is a leading e-commerce platform from Istanbul. The company raised $680 million after selling 56,740,000 American depositary shares at $12 each, the midpoint of its $11-to-$13 price range. Each ADS represents one class B ordinary share.
Lastly, Evercommerce (EVCM) also began trading. The stock opened at $20, hit a high of $21 and recently changed hands at $17.46, up nearly 3% from the offer price. Evercommerce’s IPO came in at $325 million after selling 19.1 million shares at $17, the middle of its $16-to-$18 range. The company provides SaaS software for small and midsize service businesses.
RADNOR, Pa., March 29, 2021 /PRNewswire/ — NeuroRx, Inc. today reports 60-day results of the Phase 2b/3 trial of intravenously-administered ZYESAMI™ (aviptadil acetate) for the treatment of respiratory failure in critically-ill patients with COVID-19, which is being developed in collaboration with Relief Therapeutics Holding AG (SIX:RLF,OTCQB:RLFTF). Across all patients and sites, ZYESAMI™ met the primary endpoint for successful recovery from respiratory failure at days 28 (P = .014) and 60 (P = .013) and also demonstrated a meaningful benefit in survival (P = < .001) after controlling for ventilation status and treatment site.
In addition to the robust overall significance across all 196 treated patients at all 10 clinical sites, the prespecified analysis of recovery from respiratory failure is clinically and statistically significant in the 127 patients treated by High Flow Nasal Cannula (HFNC) (P = .02), compared to those treated with mechanical or non-invasive ventilation at tertiary care hospitals. In this group, ZYESAMI™ patients had a 71% chance of successful recovery by day 28 vs. 48% in the placebo group (P = .017) and a 75% rate of successful recovery by day 60 vs. 55% in the placebo group (P = .036). Eighty-four percent (84%) of HFNC patients treated at tertiary medical centers with ZYESAMI™ survived to day 60 compared with 60% of those treated with placebo (P = .007).
To the company’s knowledge, ZYESAMI™ is the first COVID-19 therapeutic to demonstrate advantages in both survival and recovery from critical COVID-19 in a randomized, double-blind multicenter trial. On the basis of these findings, NeuroRx plans to apply immediately to the United States Food and Drug Administration (“FDA”) for Emergency Use Authorization (EUA) and to subsequently submit a New Drug Application (NDA).
Recovery from respiratory failure (without relapse) with discharge from acute care and survival through the observation period was the prespecified primary endpoint specified by FDA for the study, originally intended to be assessed at 28 days and then extended to 60 days based on recently-published FDA guidance. The above analysis includes all 196 participants who were randomized and treated in the placebo-controlled, double-blind clinical trial (www.clinicaltrials.gov NCT04311697) conducted at 10 US hospitals. Treatment with ZYESAMI™ or placebo was in addition to standard of care treatment that included steroids, convalescent plasma, antiviral therapy, anticoagulants, and various anti-cytokine drugs.
NeuroRx has announced the commencement of a clinical trial of inhaled ZYESAMI™ for the treatment of patients with moderate and severe COVID-19 with the aim of preventing progression to respiratory failure. NeuroRx has also announced the inclusion of inhaled ZYESAMI™ in the I-SPY clinical trial platform for patients with COVID-19 respiratory failure. The company has signed a clinical trial participation agreement with the National Institutes of Health.
The study’s coordinating committee, including Professors Dushyantha Jayaweera, MD, FACP (University of Miami), Richard Lee, MD, (UC Irvine), and J. Georges Youssef, MD (Houston Methodist Hospital) commented, “The 60-day observation framework implemented last month by FDA for critically ill patients with COVID-19 is more consistent with the clinical course of this lethal disease than the 28-day time frame originally adapted from other conditions that cause respiratory distress. The association of baseline oxygenation status (high flow nasal oxygen vs. ventilation) is not surprising in that patients who require mechanical or noninvasive ventilation in order to maintain blood oxygen are likely to have substantially more damage to the lining of their lungs compared to patients whose blood oxygen level can be maintained with high-flow oxygen delivered to the nose. The finding that patients fared substantially better in tertiary care centers as compared to regional hospitals may be influenced by the intensity of the public health crisis at the regional hospitals that participated in the study, all of which were operating at 200% or higher overcapacity in their intensive care units with implementation of temporary ICU beds and shortages of critical care staff.”
Prof. Jonathan Javitt, MD, MPH, Chairman and CEO of NeuroRx, said, “ZYESAMI has now demonstrated itself in a phase 2/3 trial, conducted under FDA Fast Track Designation, not only to shorten hospitalization (as was previously reported) but also to save lives and increase the likelihood of patients returning safely home to their families. In exactly 12 months, a lifesaving drug has advanced from concept to clinical success in partnership with Relief Therapeutics in the midst of a public health emergency that has claimed the lives of millions. Today’s findings confirm the often dramatic clinical success that has been seen in numerous patients treated in the US and abroad under emergency use protocols. We look forward to working with the National Institutes of Health, the Department of Defense, the FDA, and regulators around the world to bring this treatment to patients as quickly as possible.”
An investor conference call will be held today, March 29th at 8:30am EDT. Participants can dial (+1) 866-373-3402 or join via webcast at https://bit.ly/3sqPyDS. Those wishing to ask questions should submit those questions to [email protected].
NeuroRx, Inc. has signed an agreement to merge with Big Rock Acquisition Corp. Details may be viewed at http://irdirect.net/filings/viewer/index/1719406/000119312521019278/
About VIP in COVID-19 Vasoactive Intestinal Polypeptide (VIP) was first discovered by the late Dr. Sami Said in 1970. Although first identified in the lung, it was purified from the intestinal tract. VIP is now known to be produced throughout the body and to be primarily concentrated in the lungs. VIP has been shown in more than 100 peer-reviewed studies to have potent anti-inflammatory/anti-cytokine activity in animal models of respiratory distress, acute lung injury, and inflammation. Most importantly, VIP binds specifically to the alveolar type II cell (ATII) in the air sac (alveolus) of the lung. VIP stimulates ATII cells to make the surfactant that must coat the lining of the lung in order for the lung to exchange oxygen with the blood. Loss of surfactant causes respiratory failure and alveolar collapse, which is a hallmark of COVID-19.
COVID-19-related respiratory failure is caused by selective infection of the ATII cell by the SARS-CoV-2 virus. The ATII cells are vulnerable because of their (ACE2) surface receptors, which serve as the route of entry for the virus. Coronavirus infection of the ATII cell shuts down surfactant production, triggers the formation of inflammatory cytokines, and causes cell death (cytopathy). VIP is shown to upregulate surfactant production, block Coronavirus replication in the ATII cell, block cytokine synthesis, and prevent viral-induced cell death (cytopathy). To our knowledge, other than ZYESAMI™, no currently proposed treatments for COVID-19 specifically target this mechanism of action.
About NeuroRx, Inc. NeuroRx draws upon more than 100 years of collective drug development experience from senior executives of AstraZeneca, Eli Lilly, Novartis, Pfizer, and PPD. In addition to its work on Aviptadil, NeuroRx has been awarded Breakthrough Therapy Designation and a Special Protocol Agreement to develop NRX-101 in suicidal bipolar depression and is currently in Phase 3 trials. Its executive team is led by Prof. Jonathan C. Javitt, MD, MPH, who has served as a health advisor to four Presidential administrations and worked on paradigm-changing drug development projects for Merck, Allergan, Pharmacia, Pfizer, Novartis, and Mannkind, together with Robert Besthof, MIM, who served as the Global Vice President (Commercial) for Pfizer’s Neuroscience and Pain Division. NeuroRx recently announced a plan to complete a business combination with Big Rock Partners Acquisition Corp (NASDAQ:BRPA) (“BRPA”), and intends to apply for listing on the NASDAQ under the proposed symbol “NRXP”.
About Relief Therapeutics Holding AG Relief focuses primarily on clinical-stage programs based on molecules of natural origin (peptides and proteins) with a history of clinical testing and use in human patients or a strong scientific rationale. Currently, Relief is concentrating its efforts on developing new treatments for respiratory disease indications. Its lead drug candidate RLF-100™ (aviptadil) is being investigated in two placebo-controlled U.S. phase 2b/3 clinical trials in respiratory failure due to COVID-19. Relief also holds a patent issued in the United States and various other countries covering potential formulations of RLF-100™. Relief is listed on the SIX Swiss Exchange under the symbol RLF and quoted in the U.S. on OTCQB under the symbol RLFTF. www.relieftherapeutics.com.
Cautionary Note Regarding Forward Looking Statements Statements contained in this press release that are not historical facts may be forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. Forward-looking statements generally relate to future events or NeuroRx’s future financial or operating performance. In some cases, you can identify forward-looking statements because they contain words such as “may,” “will,” “should,” “expects,” “plans,” “anticipates,” “could,” “intends,” “target,” “projects,” “contemplates,” “believes,” “estimates,” “predicts,” “potential” or “continue” or the negative of these words or other similar terms or expressions that concern NeuroRx’s expectations, strategy, plans or intentions. Such forward-looking statements may relate to, among other things, the outcome of any discussions or applications for the future use of ZYESAMI, the approvals, timing, and ability to complete the proposed business combination with BRPA, and the combined company’s ability to continue listing on Nasdaq after closing the proposed business combination. Such forward-looking statements do not constitute guarantees of future performance and are subject to a variety of risks and uncertainties. NeuroRx does not undertake any obligation to update forward-looking statements as a result of new information, future events or developments or otherwise.
Additional Information and Where to Find It This press release relates to a proposed business combination and related transactions (the “Transactions”) between NeuroRx and BRPA. This press release does not constitute an offer to sell or exchange, or the solicitation of an offer to buy or exchange, any securities, nor shall there be any sale of securities in any jurisdiction in which such offer, sale or exchange would be unlawful prior to registration or qualification under the securities laws of any such jurisdiction. BRPA has filed a registration statement on Form S-4 (“Registration Statement”), which includes a preliminary proxy statement for the solicitation of the approval of BRPA’s stockholders, a preliminary prospectus for the offer and sale of BRPA’s securities in the Transactions and a preliminary consent solicitation statement of NeuroRx, and other relevant documents with the SEC. The proxy statement/prospectus/consent solicitation statement will be mailed to stockholders of NeuroRx and BRPA as of a record date to be established for voting on the proposed business combination. INVESTORS AND SECURITY HOLDERS OF NEURORX AND BRPA ARE URGED TO READ THE REGISTRATION STATEMENT, PROXY STATEMENT/PROSPECTUS/CONSENT SOLICITATION STATEMENT AND OTHER RELEVANT DOCUMENTS THAT WILL BE FILED WITH THE SEC CAREFULLY AND IN THEIR ENTIRETY WHEN THEY BECOME AVAILABLE BECAUSE THEY WILL CONTAIN IMPORTANT INFORMATION ABOUT THE PROPOSED TRANSACTIONS. Investors and security holders will be able to obtain free copies of the registration statement, proxy statement, prospectus and other documents containing important information about NeuroRx and BRPA once such documents are filed with the SEC, through the website maintained by the SEC at http://www.sec.gov. In addition, copies of the documents filed with the SEC by BRPA can be obtained free of charge on BRPA’s website at www.bigrockpartners.com or by directing a written request to BRPA at 2645 N. Federal Highway, Suite 230 Delray Beach, FL 33483.
Participants in the Solicitation NeuroRx, BRPA and their respective directors and executive officers, under SEC rules, may be deemed to be participants in the solicitation of proxies of BRPA’s stockholders in connection with the proposed Transactions. Investors and securityholders may obtain more detailed information regarding the names and interests in the proposed Transactions of NeuroRx’s and BRPA’s respective directors and officers in BRPA’s filings with the SEC, including the proxy statement/consent solicitation statement/prospectus statement. You may obtain a free copy of these documents as described in the preceding paragraph.
CORPORATE CONTACT Jonathan C. Javitt, M.D., MPH Chairman and Chief Executive Officer [email protected]
INVESTOR RELATIONS Ryan Sheffield [email protected] (484) 254-6134, ext. 723
MEDIA RELATIONS Greg Parasmo [email protected] (484) 254-6134, ext. 724
Across the world, there are multiple variants of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (Covid-19). SARS-CoV-2 variants have been classified by the Centers for Disease Control and Prevention (CDC) as variants of interest, variants of concern, and variants of high consequence. Three new variants1 that have rapidly become dominant within their countries have aroused concerns: B.1.1.7 (also known as VOC-202012/01), 501Y.V2 (B.1.351), and P.1 (B.1.1.28.1).
The B.1.1.7 variant (23 mutations with 17 amino acid changes) was first described in the United Kingdom on December 14, 2020; the 501Y.V2 variant (23 mutations with 17 amino acid changes) was initially reported in South Africa on December 18, 2020; and the P.1 variant (approximately 35 mutations with 17 amino acid changes) was reported in Brazil on January 12, 2021. By February 22, 2021, the B.1.1.7 variant had been reported in 93 countries, the 501Y.V2 variant in 45, and the P.1 variant in 21.1 All three variants have the N501Y mutation, which changes the amino acid asparagine (N) to tyrosine (Y) at position 501 in the receptor-binding domain of the spike protein. The 501Y.V2 and P.1 variants both have two additional receptor-binding–domain mutations, K417N/T and E484K. These mutations increase the binding affinity of the receptor-binding domain to the angiotensin-converting enzyme 2 (ACE2) receptor. Four key concerns stemming from the emergence of the new variants are their effects on viral transmissibility, disease severity, reinfection rates (i.e., escape from natural immunity), and vaccine effectiveness (i.e., escape from vaccine-induced immunity).
The 501Y.V2 variant spread rapidly in South Africa, accounting for 11% of the viruses sequenced (44 of 392) in the first week of October 2020, for 60% of those sequenced (302 of 505) in the first week of November 2020, and for 87% of those sequenced (363 of 415) in the first week of December 2020. In Western Cape, a South African province where the 501Y.V2 variant is predominant, a threshold of 100,000 cases of Covid-19 was reached approximately 50% more quickly in the second wave of infection than in the first wave (54 vs. 107 days). The 501Y.V2 variant has been estimated to be 50%2 more transmissible than preexisting variants in South Africa, and B.1.1.7 to be between 43% and 82%3 more transmissible than preexisting variants in the United Kingdom.
Hospital admission rates of diagnosed cases and the clinical profile of admitted patients were similar in the first and second waves in Western Cape. However, a preliminary analysis by the National Institute of Communicable Diseases showed that the 501Y.V2 variant was associated with in-hospital mortality that was 20% higher in the second wave in South Africa than in the first wave. This finding was due mainly to the greater transmissibility of this variant, which rapidly overburdened health services and thus compromised timely access to hospital care and the quality of that care. Evidence from the United Kingdom indicates that the B.1.1.7 variant may be associated with a higher risk of death than preexisting variants in the United Kingdom.4 Although there is no evidence that antiviral agents and antiinflammatory treatments are any less effective with the emerging variants than with the preexisting variants, treatment with convalescent serum and monoclonal antibodies may not be as effective.
With regard to escape from natural immunity, the B.1.1.7 variant showed a modest decrease in neutralization activity, by a factor of 1.5, whereas the 501Y.V2 variant showed complete escape from neutralizing antibodies in 48% of convalescent serum samples (21 of 44) obtained from patients who had previously had Covid-19.5 A serendipitous finding from a vaccine trial in South Africa, in which 31% of the enrolled participants had previously been infected with SARS-CoV-2, was that the incidence of Covid-19, as confirmed on polymerase chain reaction, was 7.9% among seronegative enrollees and 4.4% among seropositive enrollees in the placebo group. This finding indicates that previous infection with preexisting variants may provide only partial protection from reinfection with the 501Y.V2 variant.
Summary Results on SARS-CoV-2 Vaccine Trial Efficacy and Viral Neutralization of the B.1.1.7, P.1, and 501Y.V2 Variants, as Compared with Preexisting Variants.
With regard to escape from vaccine-induced immunity, the B.1.1.7 variant showed modest decreases in neutralizing activity in serum samples obtained from vaccinated persons (Table 1). The serum neutralizing activity for the 501Y.V2 variant among vaccinated persons was lower by a factor of 1.6 to 8.6 for the BBIBP-CorV vaccine, the BNT162b2 vaccine, and the mRNA-1273 vaccine but was lower by a factor of up to 86, including complete immune escape, for the AZD1222 vaccine (Table 1). Neutralizing activity for the P.1 variant among vaccinated persons was lower by a factor of 6.7 for the BNT162b2 vaccine and by a factor of 4.5 for the mRNA-1273 vaccine (Table 1). The clinical relevance of the lower neutralization activity for either mild or severe Covid-19 is not clear, but efficacy in clinical trials was lower for all three vaccines tested in the midst of transmission of the 501Y.V2 variant in South Africa than efficacy in trials conducted in countries with preexisting variants. Efficacy was higher by a factor of 3.2 with the AZD1222 vaccine in the United Kingdom and Brazil than in South Africa (70% vs. 22%), higher by a factor of 1.8 with the NVX-CoV237 vaccine in the United Kingdom than in South Africa (89% vs. 49%), and higher by a factor of 1.3 with the Ad26.COV2.S vaccine in the United States than in South Africa (72% vs. 57%).
The emergence of these three new variants of concern highlight the importance of vigilance with genomic surveillance for the early identification of future variants. Recently, two more SARS-CoV-2 variants, B.1.427 and B.1.429, which were first detected in California, have been shown to be approximately 20% more transmissible than preexisting variants and have been classified by the CDC as variants of concern. The potential of variants to escape naturally induced and vaccine-induced immunity makes the development of next-generation vaccines that elicit broadly neutralizing activity against current and potential future variants a priority. The suppression of viral replication with both public health measures and the equitable distribution of vaccines is critical in reducing the risk of generation of new variants.
Salim S. Abdool Karim, M.B., Ch.B., Ph.D. Centre for the AIDS Program of Research in South Africa, Durban, South Africa [email protected]
Tulio de Oliveira, Ph.D. KwaZulu-Natal Research Innovation and Sequencing Platform (KRISP), Durban, South Africa
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
This letter was published on March 24, 2021, at NEJM.org.
2. Pearson CAB, Russell TW, Davies N, et al. Estimates of severity and transmissibility of novel SARS-CoV-2 variant 501Y.V2 in South Africa. London: CMMID Repository, 2021 (https://cmmid.github.io/topics/covid19/sa-novel-variant.html).
3. Davies N, Abbott S, Barnard RC, et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. London: CMMID Repository, 2020 (https://cmmid.github.io/topics/covid19/uk-novel-variant.html).
4. Horby P, Huntley C, Davies N, et al. NERVTAG paper on COVID-19 variant of concern B.1.1.7. London: Department of Health and Social Care, Scientific Advisory Group for Emergencies, January2021 (https://www.gov.uk/government/publications/nervtag-paper-on-covid-19-variant-of-concern-b117).
5. Wibmer CK, Ayres F, Hermanus T, et al. SARS-CoV-2 501Y.V2 escapes neutralization by South African COVID-19 donor plasma. January19, 2021 (https://www.biorxiv.org/content/10.1101/2021.01.18.427166v1). preprint.
10.1056/NEJMc2100362-t1
Summary Results on SARS-CoV-2 Vaccine Trial Efficacy and Viral Neutralization of the B.1.1.7, P.1, and 501Y.V2 Variants, as Compared with Preexisting Variants.*
Vaccine (Company)
Preexisting Variants
Neutralization by Pseudovirion or Live Viral Plaque Assay
Locals who recalled hearing it back in December said they scrambled to take up the offer — 750 rupees was about twice what they’d usually earn for a day’s hard labor. And many had struggled to work at all during the pandemic.
“They told us it is the corona vaccine and we should get it so that we don’t fall sick,” said Yashoda Bai Yadav, a housewife from Bhopal who participated in the trial alongside her husband.
The Covaxin Phase 3 study, sponsored by the vaccine’s developers, Indian biotech company Bharat Biotech and the Indian Council of Medical Research (ICMR), involves almost 26,000 people at 26 locations, including more than 1,700 in Bhopal, the site of one of the world’s worst industrial disasters.
The Shankar Nagar slum — where many of the participants live — is just 3.7km (2.3 miles) from the abandoned Union Carbide factory which was at the center of the 1984 disaster that exposed more than half a million people to a toxic gas cloud. Nearly 4,000 people died in the immediate aftermath, and the disaster was blamed for at least 10,000 subsequent deaths, and more than 100,000 permanent injuries.
Decades later, many residents still suffer related health issues, raising questions from local non-governmental organizations about residents’ suitability to take part in a study that vaccine developer Bharat Biotech has called the biggest Phase 3 vaccine trial ever conducted in India.
Phase 3 trials are traditionally the final step of human trials before a vaccine is authorized to roll out en masse. However, Covaxin was approved by the Drugs Controller General of India for restricted emergency use in January, before preliminary results from the trial were released. Its Phase 3 trial isn’t expected to be completed until next year. The government has procured 5.5 million doses of Covaxin and 11 million doses of Covishield — the local name for the Oxford-AstraZeneca vaccine — for the first phase of what it is calling the largest immunization drive in the world.
At least two bioethics experts, one public health expert and four local non-governmental organizations, have raised ethical questions about the trial site in Bhopal, run by People’s Hospital, which is associated with the People’s College of Medical Sciences and Research Centre. In addition, those concerns were also raised in a joint statement released on January 14 by more than 40 organizations and 180 individuals, including public health activists and bioethicists.
More than a dozen Bhopal trial participants told CNN they did not know they were taking part in a clinical trial. Another four knew they were part of a trial, but say they did not understand what that meant.
Bharat Biotech, ICMR and People’s Hospital have all denied wrongdoing. They say that the trial complied with study protocol, guidelines and regulatory provisions, and that they are focused on generating high quality data and would not do anything that compromises patient safety. They say that participants gave informed consent and denied that the money offered acted as an incentive. India’s drug regulator, the country’s health ministry, and the ethical committee overseeing the trial in Bhopal have not commented on the allegations.
The push for Covaxin is tied up in national rhetoric, as India — already the global leader in vaccine production — aims to complete an ambitious rollout at home, and engage in vaccine diplomacy by exporting Indian-made shots. On January 16, Indian Prime Minister Narendra Modi said: “The world’s confidence in India’s scientists and our vaccine expertise is going to be further strengthened after the Made in India corona vaccines.”
But Jesani, Dr. Anant Bhan, a Bhopal-based bioethics expert, and Amulya Nidhi, a public health expert and the co-convener of the People’s Health Movement India, all say that the alleged recruitment process, if proven true, would be a violation of Indian protocols governing how vaccine trials should be conducted.
That could undermine the quality of the trial data, and potentially global trust in India’s prized coronavirus vaccine.
‘We thought it was the vaccine’
Shankar Nagar slum in Bhopal is made up of tiny, colorful houses with roofs created from tin sheets and discarded tarps.
Typically, many locals work as day laborers, waving down vans on the main road each morning to go to construction sites where they spend hours lifting stones and bricks. Since the pandemic, there hasn’t been enough work to go around, forcing many to rely on government-provided rations. Some women wander the slum, carrying sticks to sell as firewood. Others have turned to alcohol or chewing tobacco to pass the time.
So when the white van that locals recalled arrived in Bhopal slum areas near People’s Hospital offering the vaccine, 18 people saw it as a quick way to make money, they told CNN.
“My life will go anyway someday,” Hira Bai, a mother of three, said sardonically. “I went because of the greed of 750 rupees, anyway we are used to dying … my life has no value.”
Locals say they believed the van was from People’s Hospital, a private institute less than 3 kilometers (1.9 miles) away from Shankar Nagar which would often send vans to the area to conduct checkups as part of the hospital’s community outreach program. Some said they immediately piled into the vehicle, which seated more than a dozen passengers.
“The van came and everyone around me was going so I also went,” said Kesri Chillaar, 59, a laborer who lives with his wife and three children in nearby Gareeb Nagar slum.
“We thought it was the vaccine, so we went,” said Yadav, the housewife, who lives in Oriya Basti, another slum close to Shankar Nagar. “We didn’t know it was a trial.”
Chotu Das Beragi, a 27-year-old laborer, said he heard the loudspeaker announce that if he didn’t take the vaccine now, he may have to pay money for it later. “I thought, ‘There is no work anyway these days’ … so I thought, ‘Let me get the vaccine, I will get 750 rupees as well,'” he said. “I thought, ‘This will be a good way to get the day’s earnings.'”
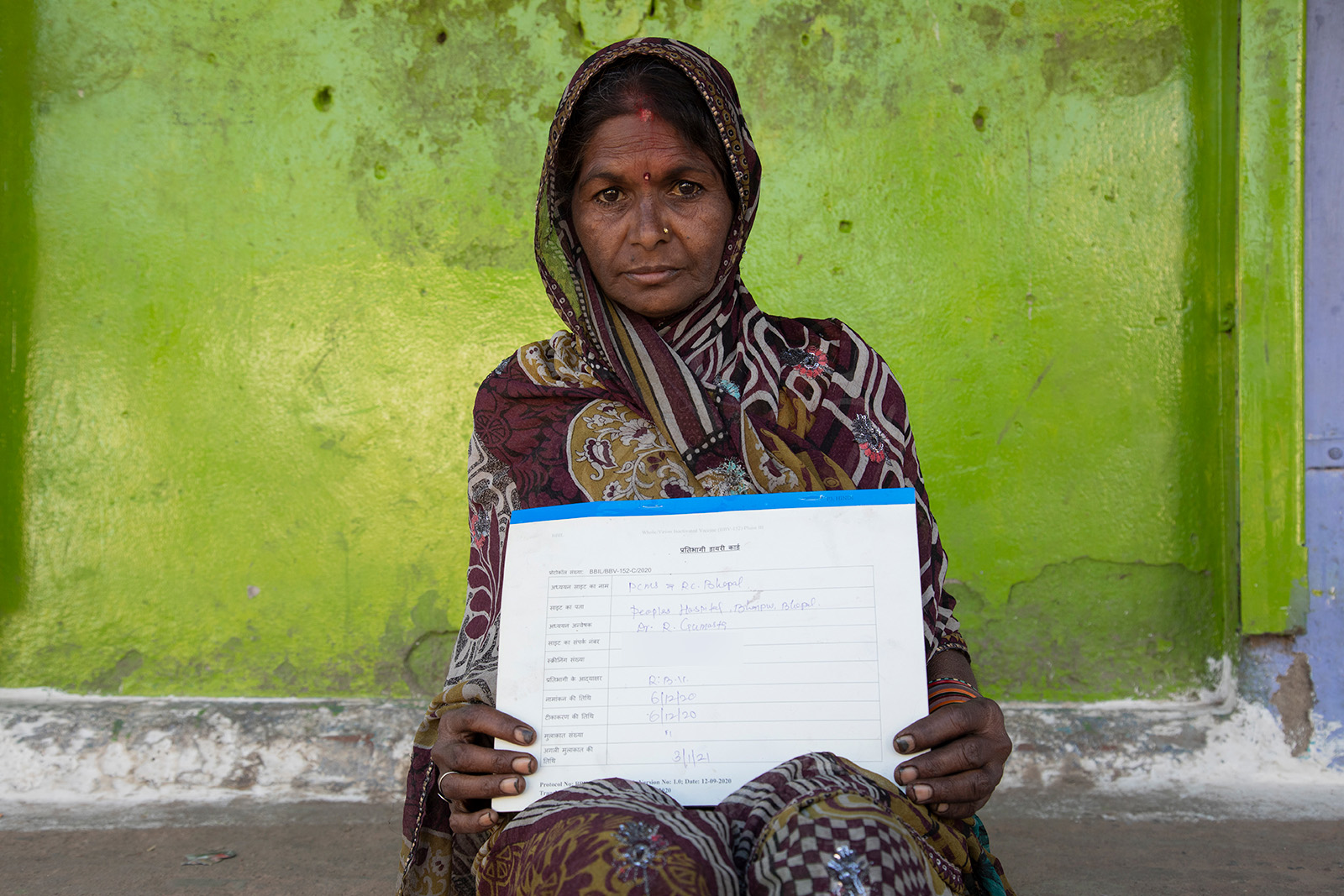
Once at the hospital, a large white building with columns and reflective blue windows, 12 participants told CNN they were asked to sign forms, although two people only signed the forms when they received their second shot. Another one gave audio-visual consent and another was asked for a thumb print instead of a signature. However, of those 14 participants, eight said that they were unable to read — the state of Madhya Pradesh, where Bhopal is located, has one of the lowest literacy rates in India at around 70%, according to the country’s most recent Census in 2011. Only participants over 60 said they were offered audio-visual consent forms. The four who could read said they weren’t given the opportunity or time to go through the 10-page form written in Hindi. The form, which CNN has obtained, includes jargon such as “immuno response,” “placebo” and “immunogenicity” — terms that would be confusing to anyone without medical training.
Although six people CNN spoke to said they were aware they were in a trial, four said they did not understand what a trial involved, or concepts such as a placebo. “I did not understand what it was a trial of,” said Beragi, the day laborer. Only two of the 21 participants CNN spoke to knew they were in a trial and had full understanding of what that entailed.
At least eight Bhopal slum residents told CNN they were not asked about underlying health conditions, even though “uncontrolled” comorbidities is listed as a reason for excluding participants in the trial’s own protocol. Rajesh Panti, 45, a survivor of the Bhopal gas tragedy, said when he received the first dose, he was not asked whether he was taking any medicine. Chillaar said he takes medication for diabetes every morning, but was not asked at the hospital whether he had any underlying health issues. Sarita Jathav, 26, said she is pregnant, but was only told that pregnant women couldn’t take the vaccine when she went to take her second dose, which she did not receive.
All 21 of the participants CNN spoke to said they were given forms to record any adverse effects of the shot. However, none had written anything on it, despite eight of the 21 participants describing side effects, including aches, vomiting, stomach issues, pains, and feeling weak. It is unclear whether the people who described side effects received the vaccine or the placebo. They said they didn’t know why recording their symptoms was important. At least 13 of the 21 participants told CNN they were illiterate, meaning they were unable to use the form anyway.
Radha Bai (top), Jetender Veria (left) and Man Singh Parihar (right) pictured in Shankar Nagar, a slum in Bhopal, India, on February 7, 2021. All say they did not realize they were participants in Phase 3 Covaxin trials. (Credit: Ajay Bedi/CNN)
Anil Kumar Dixit, the dean of People’s College of Medical Sciences and Research Centre in Bhopal, said he was not aware of any van and did not send one to the slums. He said it was clarified to participants that they were part of a trial, and that only 50% would receive the vaccine while the other half would be given a placebo. He said the hospital did pay participants 750 rupees, per the ICMR and Bharat Biotech’s instructions, but it was to cover them for any lost wages — not as an incentive to take part in the trial.
Under ICMR’s 2017 Ethical Guidelines, subjects may be paid for their inconvenience and reimbursed for expenses incurred, although not to such an extent that it induces them to take part.
Dixit said his hospital did not ask participants if they were Bhopal gas victims, although administrators did examine them for underlying health conditions and rejected them if they had a chronic health problem. Bhan, the Bhopal-based bioethics expert, said he was surprised the hospital hadn’t considered that some participants might be victims of the Bhopal gas tragedy.
Around 10% of all Bhopal participants reported minor adverse effects, while around 1 to 2% were treated in hospital, according to Dixit. He said his hospital was only registering adverse events that required treatment, and that most of the minor events had been resolved over the phone.
Dixit said that for those who couldn’t read, the form was explained in either Hindi or English, depending on what they preferred, before they signed.
Staff from People’s Hospital which is administering the trial told participants they would check up on them via phone, according to Dixit and the participants, but two participants CNN spoke to said they hadn’t received a call, and two said they didn’t know if they had. Another participant said they had received calls in the first week, but not in the second week when their adverse effects started.
Two others said they had received calls but that their phone belonged to a family member, making communication harder.
Four people CNN spoke to said they needed to go to a hospital for treatment, and of those two said they were asked to pay for treatment for what they considered adverse effects, including neck pains and vomiting, despite the 10-page document that they signed stating that they would be covered, something that is also required by India’s Good Clinical Practice guidelines.
Chillaar, for instance, said that when hospital administrators called to check on him following the shot, he told them that he was having neck problems. They told him to come in for treatment, but when he did, he said he was told to pay more than 3,000 rupees ($41). Dixit, dean of People’s College of Medical Sciences and Research Centre, said there were only “one or two cases” where miscommunication led to participants being charged.
Chillaar says he got the first shot on December 10 and the second on January 7 — Covaxin requires two shots administered four weeks apart. When he spoke to CNN on January 28, he said that he was still not able to work. “I am the primary earner and it has come to the point where we are going hungry,” he said. “I am not even able to go earn and I have spent 3,000 to 4,000 rupees on treatment.” CNN has no evidence that the shot caused his health issues and it is unclear whether he received the placebo or vaccine as the trial is blinded.
What the rules say
Hundreds of people who live in the Shankar Nagar slum still live with health effects from the Bhopal gas tragedy, according to Rachna Dhingra, the leader of Bhopal Group for Information and Action (BGIA), which works with communities impacted by groundwater contamination from the leak.
In late December, Dhingra says she began hearing reports of people living in the slum being given the coronavirus vaccine. That set off alarm bells: she knew India hadn’t yet formally rolled out a coronavirus vaccine.
Dhingrabegan investigating and found that many of those people had actually been part of a clinical vaccine trial — and many said they did not realize it.
Dhingra and BGIA spoke to 233 participants, and estimate that 800 residents from more than five slum communities impacted by the 1984 tragedy in Bhopal had been part of the Phase 3 clinical trial. Nasreen, a field worker from BGIA who uses only one name, said that in many cases entire households of five or six people had taken part in the trial.
Dhingra says in all of the cases there were issues around how consent had been obtained.
“It spread like wildfire because people thought they were not only getting vaccinated, but also that they were getting money,” Dhingra said. “They could never do this kind of announcement in middle-class neighborhoods because everyone would know that this is not possible.”
India’s New Drugs and Clinical Trials Rules 2019 require “freely given, informed, written consent” from each study subject, including that they understand the risks and responsibilities involved in receiving an unapproved drug. Information must be provided verbally and in a patient information sheet in “language that is nontechnical and understandable by the study subject.”
In the case of Covaxin, the vaccine had only been tested on approximately 755 people across both Phase 1 and 2 trials before it was administered in Phase 3 clinical trials — and those Phase 1 results, which were released in the Lancet in January, were not out when many of the participants received their first dose. That study found that the vaccine can produce antibodies to coronavirus and no serious adverse events related to the vaccine were reported.
ICMR’s head scientist of the division of epidemiology and communicable diseases, Dr. Samiran Panda, said the seriousness of the pandemic justified using the accelerated approval process without cutting any corners when it came to safety.
Dhingra also says around 25% of the participants the NGO spoke to reported experiencing adverse effects — more than twice the number that Dixit said had suffered minor adverse effects. In trials across the world, it is common for participants to report some adverse effects during a trial.
One Bhopal trial participant who died nine days after receiving the injection has drawn widespread media attention in India, prompting outlets to publish stories raising questions over the trial.
CNN has no evidence that 45-year-old Deepak Marawi’s death was linked to the vaccine trial, but because of the lack of transparency around his death — the post-mortem still hasn’t been made public — his widow, Vaijayanti Marawi, and others following the trial say the case raises concern and requires further examination. Bharat Biotech could not confirm if Marawi received the vaccine or placebo as the study is blinded, but they said his death “had been thoroughly investigated” and found not to be connected to the trial. The company says Marawi died from cardiorespiratory failure as a result of suspected poisoning.
Dixit said staff had followed up with Marawi for seven days, as he said they do with all participants, to ask about any problems. Marawi had said no every day, Dixit said.
Vaijayanti Marawi and two of her sons in Bhopal, India, on February 7, 2021. Marawi’s husband Deepak Marawi died in December after participating in the Phase 3 clinical trials.
Arun Shrivastav, the head of the pharmacology department at the Gandhi Medical College in Bhopal, which headed the investigation into Marawi’s death, said that his committee’s investigation found that the trial protocols had been adequately followed. When asked generally about the alleged use of vans in recruitment, he said that if a van loudspeaker was used to advertise the vaccine for 750 rupees, then it would be “unethical, totally wrong.”
“If there is anything like this happening then it cannot be counted in the trial and the trial would be barred,” he said.
‘Violation of good clinical practices’
Bioethics and public health experts Bhan, Jesani and Nidhi all said Bhopal residents should have been considered vulnerable, and extra care should have been taken to ensure they knew what they were agreeing to.
The standard for getting consent is even higher for vulnerable communities — including people who are impoverished or illiterate. According to India’s 2019 New Drugs and Clinical Trials rules, if a trial participant is unable to read or write, an impartial witness should be present throughout the entire informed consent process to help sign the consent form. An audio-video recording of the informed consent process is required in cases using “vulnerable subjects,” which includes “impoverished persons” and patients with incurable diseases.
“You are dealing with people who are highly vulnerable, who are not even fully educated, do you expect them to come and say, ‘These are my rights’?” said Jesani, the editor of the Indian Journal of Medical Ethics. “You have to inform them about their rights.”
As for the offer of 750 rupees, Bhan, the Bhopal-based bioethics expert, said it was not necessarily an ethical violation for money to be offered — the issue is whether it was used as an incentive.
But statements made by participants suggest that even though the amount offered was relatively low, it was enough to motivate some trial participants in Bhopal. Madhya Pradesh, where Bhopal is located, has some of the lowest wages for casual workers in India, according to a 2018 India Wage Report by the International Labour Organization. “I thought it was some patriotic thing and, I won’t lie, we were getting money also,” said Bhopal resident Panti.
If the allegations about misleading participants, failing to get informed consent and failing to follow up on adverse events are true, the problem goes beyond ethics — it reflects on the quality of the trial data, according to experts.
Bhan said that if adverse events were missed, that meant crucial data points had been left out of the Phase 3 trials.
“If that is what has happened, it’s obviously a violation of good clinical practices. It’s also a violation of guidelines around how ethical conduct of research should happen,” he said, speaking about the allegations.
The current guidelines for clinical tests in India are relatively new. After Delhi liberalized its clinical trial policy in 2005, international companies rushed to test their drugs in India, where it was cheaper and easier to find participants. Some of the tests were reportedly carried out in Bhopal, on residents who allegedly weren’t aware they were involved in trials. The 2019 New Drugs and Clinical Trials Rules are a result of various orders from the Supreme Court following a case filed in 2012 by non-profit Swasthya Adhikar Manch, which Nidhi is also a co-convener of.
Bhan, Jesani and Nidhi believe the new Bhopal allegations, if true, suggest that more work needs to be done to improve oversight over clinical trials.
Jesani says, if the allegations are founded, it means the data from Bhopal should be excluded as the trial on that site wouldn’t have been done in a scientific way.
What can be done
On January 10, Dhingra and three other Bhopal-based NGOs wrote a letter to Indian Prime Minister Narendra Modi and Health Minister Harsh Vardhan, asking them to stop the Bhopal trial. They wrote that the involvement of the Indian Council of Medical Research in a trial with “glaring and grave violations” of the guidelines ICMR laid down was “alarming and deeply troubling” and said the situation must be addressed to avoid the public losing faith in vaccines.
A timeline of Covaxin
Bharat Biotech receives Drugs Controller General of India approval to conduct Phase 3 clinical trials with 26,000 participants for Covaxin.
Covaxin’s Phase 3 clinical trials begins.
Bharat Biotech announces it has recruited 13,000 participants — around half its target.
Central government’s subject expert committee, which recommends vaccines for emergency approval, says that Bharat Biotech should try to expedite recruitment for Phase 3 Covaxin trials as “efficacy is yet to be demonstrated.”
The subject expert committee recommends India’s drug regulator approve Covaxin for restricted emergency use, citing “updated data … in the wake of the incidence of new mutated corona virus infection.”
India’s drug regulator gives restricted emergency use authorization to Covaxin and Covishield, the name given to the Oxford-AstraZeneca developed vaccine in India.
Bharat Biotech announces that it has finished recruitment and all 26,000 participants have received their first dose.
Four Bhopal-based NGOs write to India’s prime minister and health minister, warning them of alleged ethical violations in the Bhopal Phase 3 Covaxin trials.
India begins the first phase of its vaccination drive — rolling out Covaxin and Covishield to 10 million healthcare workers.
Source: CNN reporting
They copied the letter to the Drugs Controller General of India, which has the power to investigate alleged breaches.
More than a month later, the groups say they have received no response.
Despite multiple requests for comment, Bharat Biotech has not responded to CNN’s emailed questions. In a public statement in January, the company said participation was voluntary and every participant gave fully informed consent, even those who were not able to read or write. All participants were paid 750 rupees, but it was not an inducement, the company said, rather a payment to cover transport and expenses, adding that they are following practices set by the Indian Good Clinical Practice guidelines. Participants are only enrolled after a careful assessment of their “various health parameters,” the company said.
“The development of Covaxin is a matter of great pride to us, not just at Bharat Biotech but also for India, and indeed the rest of the world,” the company said. “We would not do anything that would compromise either the scientific rigor of what we do or the lives of patients.”
“Our constant focus during the development of the vaccine and the clinical trials has been on ensuring patient safety and ensuring that the study is done to the requirements of all the relevant and applicable rules and guidelines, and that the data generated is of the highest quality and valid.”
Three other trial sites told CNN they had collected data on all minor adverse events, including headaches or fever.
Four trial sites told CNN they had difficulty reaching the target of 1,000 trial participants. By contrast, the People’s Hospital site in Bhopal managed to register cases quickly. “Other centers were not able to achieve the target so then (Bharat Biotech) asked us to do more numbers,” Dixit said.
ICMR’s head scientist of the division of epidemiology and communicable diseases, Panda, said excluding the Bhopal gas victims from the study would have been discriminatory, denying them an “opportunity.”
“You are dealing with people who are highly vulnerable, who are not even fully educated, do you expect them to come and say, ‘These are my rights’?” Amar Jesani
Panda said the ICMR spoke to the principal investigator running the Bhopal trial following the ethical violation allegations in the media, but were assured by the investigator and his medical team that they had followed protocol. They did not independently speak to any of the participants in the trial, although they kept the Drugs Controller informed of their Bhopal communications, Panda said.
According to Panda, there have been no allegations of wrongdoing at any other site. CNN has contacted 12 other sites but has found no evidence that the alleged issues that happened in Bhopal took place at other sites.
According to Dr. Mohammad Shameem, the principal investigator of a Phase 3 Covaxin trial site in Uttar Pradesh, Bhopal’s alleged recruitment strategy of offering vaccines for 750 rupees using a van with a loudspeaker would have needed sign-off from the local ethical committee. It’s not clear if the People’s Hospital’s institutional ethics committee knew that a van was allegedly being used for promotional purposes. CNN has attempted to contact the committee for comment.
Push to roll out
The controversy over the Covaxin trials is taking place as India rolls out its ambitious plan to immunize 300 million of its 1.3 billion population by August.
But some healthcare workers in India, who were first in line to receive a shot, have expressed reticence to take the vaccine until there is more data on Covaxin.
Experts worry the ethical questions over Bhopal could undermine trust in the vaccine when it’s rolled out more broadly — both in India and abroad.
Bharat Biotech has signed an agreement to supply Brazil with the vaccine, and is applying to conduct trials in Bangladesh, Reuters reported. Bharat Biotech also signed an agreement with biopharmaceutical company Ocugen to develop its vaccine for the US market.
India has traditionally been receptive to vaccines, and there isn’t a strong anti-vaccination movement in the country, but Jesani, from the Indian Journal of Medical Ethics, says that could change if the government doesn’t act to restore confidence in Covaxin. Bhan, the bioethics expert, said an audit of the Bhopal trial would build confidence in the process.
If these initial questions linger and manifest as general anti-vaccination sentiment, that could be a problem for the public’s willingness not only to get the Covaxin vaccine, but also other coronavirus vaccines as India continues to report more than 10,000 cases each day.
Jesani said that is why it is so crucial that authorities investigate claims that some Bhopal participants didn’t know they were part of a trial.
“We don’t want people to lose faith. We don’t want people to lose trust in the vaccination,” he said. “If they lose trust in the Covid vaccine, they will lose trust in other vaccines.”
Esha Mitra reported from New Delhi and Bhopal, India. Julia Hollingsworth reported and wrote from Hong Kong. Additional reporting: Anup Dutta Photos and video: Ajay Bedi Graphics: Natalie Leung Editors: Hilary Whiteman and Jenni Marsh
Locals who recalled hearing it back in December said they scrambled to take up the offer — 750 rupees was about twice what they’d usually earn for a day’s hard labor. And many had struggled to work at all during the pandemic.
“They told us it is the corona vaccine and we should get it so that we don’t fall sick,” said Yashoda Bai Yadav, a housewife from Bhopal who participated in the trial alongside her husband.
The Covaxin Phase 3 study, sponsored by the vaccine’s developers, Indian biotech company Bharat Biotech and the Indian Council of Medical Research (ICMR), involves almost 26,000 people at 26 locations, including more than 1,700 in Bhopal, the site of one of the world’s worst industrial disasters.
The Shankar Nagar slum — where many of the participants live — is just 3.7km (2.3 miles) from the abandoned Union Carbide factory which was at the center of the 1984 disaster that exposed more than half a million people to a toxic gas cloud. Nearly 4,000 people died in the immediate aftermath, and the disaster was blamed for at least 10,000 subsequent deaths, and more than 100,000 permanent injuries.
Decades later, many residents still suffer related health issues, raising questions from local non-governmental organizations about residents’ suitability to take part in a study that vaccine developer Bharat Biotech has called the biggest Phase 3 vaccine trial ever conducted in India.
Phase 3 trials are traditionally the final step of human trials before a vaccine is authorized to roll out en masse. However, Covaxin was approved by the Drugs Controller General of India for restricted emergency use in January, before preliminary results from the trial were released. Its Phase 3 trial isn’t expected to be completed until next year. The government has procured 5.5 million doses of Covaxin and 11 million doses of Covishield — the local name for the Oxford-AstraZeneca vaccine — for the first phase of what it is calling the largest immunization drive in the world.
At least two bioethics experts, one public health expert and four local non-governmental organizations, have raised ethical questions about the trial site in Bhopal, run by People’s Hospital, which is associated with the People’s College of Medical Sciences and Research Centre. In addition, those concerns were also raised in a joint statement released on January 14 by more than 40 organizations and 180 individuals, including public health activists and bioethicists.
More than a dozen Bhopal trial participants told CNN they did not know they were taking part in a clinical trial. Another four knew they were part of a trial, but say they did not understand what that meant.
Bharat Biotech, ICMR and People’s Hospital have all denied wrongdoing. They say that the trial complied with study protocol, guidelines and regulatory provisions, and that they are focused on generating high quality data and would not do anything that compromises patient safety. They say that participants gave informed consent and denied that the money offered acted as an incentive. India’s drug regulator, the country’s health ministry, and the ethical committee overseeing the trial in Bhopal have not commented on the allegations.
The push for Covaxin is tied up in national rhetoric, as India — already the global leader in vaccine production — aims to complete an ambitious rollout at home, and engage in vaccine diplomacy by exporting Indian-made shots. On January 16, Indian Prime Minister Narendra Modi said: “The world’s confidence in India’s scientists and our vaccine expertise is going to be further strengthened after the Made in India corona vaccines.”
But Jesani, Dr. Anant Bhan, a Bhopal-based bioethics expert, and Amulya Nidhi, a public health expert and the co-convener of the People’s Health Movement India, all say that the alleged recruitment process, if proven true, would be a violation of Indian protocols governing how vaccine trials should be conducted.
That could undermine the quality of the trial data, and potentially global trust in India’s prized coronavirus vaccine.
‘We thought it was the vaccine’
Shankar Nagar slum in Bhopal is made up of tiny, colorful houses with roofs created from tin sheets and discarded tarps.
Typically, many locals work as day laborers, waving down vans on the main road each morning to go to construction sites where they spend hours lifting stones and bricks. Since the pandemic, there hasn’t been enough work to go around, forcing many to rely on government-provided rations. Some women wander the slum, carrying sticks to sell as firewood. Others have turned to alcohol or chewing tobacco to pass the time.
So when the white van that locals recalled arrived in Bhopal slum areas near People’s Hospital offering the vaccine, 18 people saw it as a quick way to make money, they told CNN.
“My life will go anyway someday,” Hira Bai, a mother of three, said sardonically. “I went because of the greed of 750 rupees, anyway we are used to dying … my life has no value.”
Locals say they believed the van was from People’s Hospital, a private institute less than 3 kilometers (1.9 miles) away from Shankar Nagar which would often send vans to the area to conduct checkups as part of the hospital’s community outreach program. Some said they immediately piled into the vehicle, which seated more than a dozen passengers.
“The van came and everyone around me was going so I also went,” said Kesri Chillaar, 59, a laborer who lives with his wife and three children in nearby Gareeb Nagar slum.
“We thought it was the vaccine, so we went,” said Yadav, the housewife, who lives in Oriya Basti, another slum close to Shankar Nagar. “We didn’t know it was a trial.”
Chotu Das Beragi, a 27-year-old laborer, said he heard the loudspeaker announce that if he didn’t take the vaccine now, he may have to pay money for it later. “I thought, ‘There is no work anyway these days’ … so I thought, ‘Let me get the vaccine, I will get 750 rupees as well,'” he said. “I thought, ‘This will be a good way to get the day’s earnings.'”
Once at the hospital, a large white building with columns and reflective blue windows, 12 participants told CNN they were asked to sign forms, although two people only signed the forms when they received their second shot. Another one gave audio-visual consent and another was asked for a thumb print instead of a signature. However, of those 14 participants, eight said that they were unable to read — the state of Madhya Pradesh, where Bhopal is located, has one of the lowest literacy rates in India at around 70%, according to the country’s most recent Census in 2011. Only participants over 60 said they were offered audio-visual consent forms. The four who could read said they weren’t given the opportunity or time to go through the 10-page form written in Hindi. The form, which CNN has obtained, includes jargon such as “immuno response,” “placebo” and “immunogenicity” — terms that would be confusing to anyone without medical training.
Although six people CNN spoke to said they were aware they were in a trial, four said they did not understand what a trial involved, or concepts such as a placebo. “I did not understand what it was a trial of,” said Beragi, the day laborer. Only two of the 21 participants CNN spoke to knew they were in a trial and had full understanding of what that entailed.
At least eight Bhopal slum residents told CNN they were not asked about underlying health conditions, even though “uncontrolled” comorbidities is listed as a reason for excluding participants in the trial’s own protocol. Rajesh Panti, 45, a survivor of the Bhopal gas tragedy, said when he received the first dose, he was not asked whether he was taking any medicine. Chillaar said he takes medication for diabetes every morning, but was not asked at the hospital whether he had any underlying health issues. Sarita Jathav, 26, said she is pregnant, but was only told that pregnant women couldn’t take the vaccine when she went to take her second dose, which she did not receive.
All 21 of the participants CNN spoke to said they were given forms to record any adverse effects of the shot. However, none had written anything on it, despite eight of the 21 participants describing side effects, including aches, vomiting, stomach issues, pains, and feeling weak. It is unclear whether the people who described side effects received the vaccine or the placebo. They said they didn’t know why recording their symptoms was important. At least 13 of the 21 participants told CNN they were illiterate, meaning they were unable to use the form anyway.
Radha Bai (top), Jetender Veria (left) and Man Singh Parihar (right) pictured in Shankar Nagar, a slum in Bhopal, India, on February 7, 2021. All say they did not realize they were participants in Phase 3 Covaxin trials. (Credit: Ajay Bedi/CNN)
Anil Kumar Dixit, the dean of People’s College of Medical Sciences and Research Centre in Bhopal, said he was not aware of any van and did not send one to the slums. He said it was clarified to participants that they were part of a trial, and that only 50% would receive the vaccine while the other half would be given a placebo. He said the hospital did pay participants 750 rupees, per the ICMR and Bharat Biotech’s instructions, but it was to cover them for any lost wages — not as an incentive to take part in the trial.
Under ICMR’s 2017 Ethical Guidelines, subjects may be paid for their inconvenience and reimbursed for expenses incurred, although not to such an extent that it induces them to take part.
Dixit said his hospital did not ask participants if they were Bhopal gas victims, although administrators did examine them for underlying health conditions and rejected them if they had a chronic health problem. Bhan, the Bhopal-based bioethics expert, said he was surprised the hospital hadn’t considered that some participants might be victims of the Bhopal gas tragedy.
Around 10% of all Bhopal participants reported minor adverse effects, while around 1 to 2% were treated in hospital, according to Dixit. He said his hospital was only registering adverse events that required treatment, and that most of the minor events had been resolved over the phone.
Dixit said that for those who couldn’t read, the form was explained in either Hindi or English, depending on what they preferred, before they signed.
Staff from People’s Hospital which is administering the trial told participants they would check up on them via phone, according to Dixit and the participants, but two participants CNN spoke to said they hadn’t received a call, and two said they didn’t know if they had. Another participant said they had received calls in the first week, but not in the second week when their adverse effects started.
Two others said they had received calls but that their phone belonged to a family member, making communication harder.
Four people CNN spoke to said they needed to go to a hospital for treatment, and of those two said they were asked to pay for treatment for what they considered adverse effects, including neck pains and vomiting, despite the 10-page document that they signed stating that they would be covered, something that is also required by India’s Good Clinical Practice guidelines.
Chillaar, for instance, said that when hospital administrators called to check on him following the shot, he told them that he was having neck problems. They told him to come in for treatment, but when he did, he said he was told to pay more than 3,000 rupees ($41). Dixit, dean of People’s College of Medical Sciences and Research Centre, said there were only “one or two cases” where miscommunication led to participants being charged.
Chillaar says he got the first shot on December 10 and the second on January 7 — Covaxin requires two shots administered four weeks apart. When he spoke to CNN on January 28, he said that he was still not able to work. “I am the primary earner and it has come to the point where we are going hungry,” he said. “I am not even able to go earn and I have spent 3,000 to 4,000 rupees on treatment.” CNN has no evidence that the shot caused his health issues and it is unclear whether he received the placebo or vaccine as the trial is blinded.
What the rules say
Hundreds of people who live in the Shankar Nagar slum still live with health effects from the Bhopal gas tragedy, according to Rachna Dhingra, the leader of Bhopal Group for Information and Action (BGIA), which works with communities impacted by groundwater contamination from the leak.
In late December, Dhingra says she began hearing reports of people living in the slum being given the coronavirus vaccine. That set off alarm bells: she knew India hadn’t yet formally rolled out a coronavirus vaccine.
Dhingrabegan investigating and found that many of those people had actually been part of a clinical vaccine trial — and many said they did not realize it.
Dhingra and BGIA spoke to 233 participants, and estimate that 800 residents from more than five slum communities impacted by the 1984 tragedy in Bhopal had been part of the Phase 3 clinical trial. Nasreen, a field worker from BGIA who uses only one name, said that in many cases entire households of five or six people had taken part in the trial.
Dhingra says in all of the cases there were issues around how consent had been obtained.
“It spread like wildfire because people thought they were not only getting vaccinated, but also that they were getting money,” Dhingra said. “They could never do this kind of announcement in middle-class neighborhoods because everyone would know that this is not possible.”
India’s New Drugs and Clinical Trials Rules 2019 require “freely given, informed, written consent” from each study subject, including that they understand the risks and responsibilities involved in receiving an unapproved drug. Information must be provided verbally and in a patient information sheet in “language that is nontechnical and understandable by the study subject.”
In the case of Covaxin, the vaccine had only been tested on approximately 755 people across both Phase 1 and 2 trials before it was administered in Phase 3 clinical trials — and those Phase 1 results, which were released in the Lancet in January, were not out when many of the participants received their first dose. That study found that the vaccine can produce antibodies to coronavirus and no serious adverse events related to the vaccine were reported.
ICMR’s head scientist of the division of epidemiology and communicable diseases, Dr. Samiran Panda, said the seriousness of the pandemic justified using the accelerated approval process without cutting any corners when it came to safety.
Dhingra also says around 25% of the participants the NGO spoke to reported experiencing adverse effects — more than twice the number that Dixit said had suffered minor adverse effects. In trials across the world, it is common for participants to report some adverse effects during a trial.
One Bhopal trial participant who died nine days after receiving the injection has drawn widespread media attention in India, prompting outlets to publish stories raising questions over the trial.
CNN has no evidence that 45-year-old Deepak Marawi’s death was linked to the vaccine trial, but because of the lack of transparency around his death — the post-mortem still hasn’t been made public — his widow, Vaijayanti Marawi, and others following the trial say the case raises concern and requires further examination. Bharat Biotech could not confirm if Marawi received the vaccine or placebo as the study is blinded, but they said his death “had been thoroughly investigated” and found not to be connected to the trial. The company says Marawi died from cardiorespiratory failure as a result of suspected poisoning.
Dixit said staff had followed up with Marawi for seven days, as he said they do with all participants, to ask about any problems. Marawi had said no every day, Dixit said.
Vaijayanti Marawi and two of her sons in Bhopal, India, on February 7, 2021. Marawi’s husband Deepak Marawi died in December after participating in the Phase 3 clinical trials.
Arun Shrivastav, the head of the pharmacology department at the Gandhi Medical College in Bhopal, which headed the investigation into Marawi’s death, said that his committee’s investigation found that the trial protocols had been adequately followed. When asked generally about the alleged use of vans in recruitment, he said that if a van loudspeaker was used to advertise the vaccine for 750 rupees, then it would be “unethical, totally wrong.”
“If there is anything like this happening then it cannot be counted in the trial and the trial would be barred,” he said.
‘Violation of good clinical practices’
Bioethics and public health experts Bhan, Jesani and Nidhi all said Bhopal residents should have been considered vulnerable, and extra care should have been taken to ensure they knew what they were agreeing to.
The standard for getting consent is even higher for vulnerable communities — including people who are impoverished or illiterate. According to India’s 2019 New Drugs and Clinical Trials rules, if a trial participant is unable to read or write, an impartial witness should be present throughout the entire informed consent process to help sign the consent form. An audio-video recording of the informed consent process is required in cases using “vulnerable subjects,” which includes “impoverished persons” and patients with incurable diseases.
“You are dealing with people who are highly vulnerable, who are not even fully educated, do you expect them to come and say, ‘These are my rights’?” said Jesani, the editor of the Indian Journal of Medical Ethics. “You have to inform them about their rights.”
As for the offer of 750 rupees, Bhan, the Bhopal-based bioethics expert, said it was not necessarily an ethical violation for money to be offered — the issue is whether it was used as an incentive.
But statements made by participants suggest that even though the amount offered was relatively low, it was enough to motivate some trial participants in Bhopal. Madhya Pradesh, where Bhopal is located, has some of the lowest wages for casual workers in India, according to a 2018 India Wage Report by the International Labour Organization. “I thought it was some patriotic thing and, I won’t lie, we were getting money also,” said Bhopal resident Panti.
If the allegations about misleading participants, failing to get informed consent and failing to follow up on adverse events are true, the problem goes beyond ethics — it reflects on the quality of the trial data, according to experts.
Bhan said that if adverse events were missed, that meant crucial data points had been left out of the Phase 3 trials.
“If that is what has happened, it’s obviously a violation of good clinical practices. It’s also a violation of guidelines around how ethical conduct of research should happen,” he said, speaking about the allegations.
The current guidelines for clinical tests in India are relatively new. After Delhi liberalized its clinical trial policy in 2005, international companies rushed to test their drugs in India, where it was cheaper and easier to find participants. Some of the tests were reportedly carried out in Bhopal, on residents who allegedly weren’t aware they were involved in trials. The 2019 New Drugs and Clinical Trials Rules are a result of various orders from the Supreme Court following a case filed in 2012 by non-profit Swasthya Adhikar Manch, which Nidhi is also a co-convener of.
Bhan, Jesani and Nidhi believe the new Bhopal allegations, if true, suggest that more work needs to be done to improve oversight over clinical trials.
Jesani says, if the allegations are founded, it means the data from Bhopal should be excluded as the trial on that site wouldn’t have been done in a scientific way.
What can be done
On January 10, Dhingra and three other Bhopal-based NGOs wrote a letter to Indian Prime Minister Narendra Modi and Health Minister Harsh Vardhan, asking them to stop the Bhopal trial. They wrote that the involvement of the Indian Council of Medical Research in a trial with “glaring and grave violations” of the guidelines ICMR laid down was “alarming and deeply troubling” and said the situation must be addressed to avoid the public losing faith in vaccines.
A timeline of Covaxin
Bharat Biotech receives Drugs Controller General of India approval to conduct Phase 3 clinical trials with 26,000 participants for Covaxin.
Covaxin’s Phase 3 clinical trials begins.
Bharat Biotech announces it has recruited 13,000 participants — around half its target.
Central government’s subject expert committee, which recommends vaccines for emergency approval, says that Bharat Biotech should try to expedite recruitment for Phase 3 Covaxin trials as “efficacy is yet to be demonstrated.”
The subject expert committee recommends India’s drug regulator approve Covaxin for restricted emergency use, citing “updated data … in the wake of the incidence of new mutated corona virus infection.”
India’s drug regulator gives restricted emergency use authorization to Covaxin and Covishield, the name given to the Oxford-AstraZeneca developed vaccine in India.
Bharat Biotech announces that it has finished recruitment and all 26,000 participants have received their first dose.
Four Bhopal-based NGOs write to India’s prime minister and health minister, warning them of alleged ethical violations in the Bhopal Phase 3 Covaxin trials.
India begins the first phase of its vaccination drive — rolling out Covaxin and Covishield to 10 million healthcare workers.
Source: CNN reporting
They copied the letter to the Drugs Controller General of India, which has the power to investigate alleged breaches.
More than a month later, the groups say they have received no response.
Despite multiple requests for comment, Bharat Biotech has not responded to CNN’s emailed questions. In a public statement in January, the company said participation was voluntary and every participant gave fully informed consent, even those who were not able to read or write. All participants were paid 750 rupees, but it was not an inducement, the company said, rather a payment to cover transport and expenses, adding that they are following practices set by the Indian Good Clinical Practice guidelines. Participants are only enrolled after a careful assessment of their “various health parameters,” the company said.
“The development of Covaxin is a matter of great pride to us, not just at Bharat Biotech but also for India, and indeed the rest of the world,” the company said. “We would not do anything that would compromise either the scientific rigor of what we do or the lives of patients.”
“Our constant focus during the development of the vaccine and the clinical trials has been on ensuring patient safety and ensuring that the study is done to the requirements of all the relevant and applicable rules and guidelines, and that the data generated is of the highest quality and valid.”
Three other trial sites told CNN they had collected data on all minor adverse events, including headaches or fever.
Four trial sites told CNN they had difficulty reaching the target of 1,000 trial participants. By contrast, the People’s Hospital site in Bhopal managed to register cases quickly. “Other centers were not able to achieve the target so then (Bharat Biotech) asked us to do more numbers,” Dixit said.
ICMR’s head scientist of the division of epidemiology and communicable diseases, Panda, said excluding the Bhopal gas victims from the study would have been discriminatory, denying them an “opportunity.”
“You are dealing with people who are highly vulnerable, who are not even fully educated, do you expect them to come and say, ‘These are my rights’?” Amar Jesani
Panda said the ICMR spoke to the principal investigator running the Bhopal trial following the ethical violation allegations in the media, but were assured by the investigator and his medical team that they had followed protocol. They did not independently speak to any of the participants in the trial, although they kept the Drugs Controller informed of their Bhopal communications, Panda said.
According to Panda, there have been no allegations of wrongdoing at any other site. CNN has contacted 12 other sites but has found no evidence that the alleged issues that happened in Bhopal took place at other sites.
According to Dr. Mohammad Shameem, the principal investigator of a Phase 3 Covaxin trial site in Uttar Pradesh, Bhopal’s alleged recruitment strategy of offering vaccines for 750 rupees using a van with a loudspeaker would have needed sign-off from the local ethical committee. It’s not clear if the People’s Hospital’s institutional ethics committee knew that a van was allegedly being used for promotional purposes. CNN has attempted to contact the committee for comment.
Push to roll out
The controversy over the Covaxin trials is taking place as India rolls out its ambitious plan to immunize 300 million of its 1.3 billion population by August.
But some healthcare workers in India, who were first in line to receive a shot, have expressed reticence to take the vaccine until there is more data on Covaxin.
Experts worry the ethical questions over Bhopal could undermine trust in the vaccine when it’s rolled out more broadly — both in India and abroad.
Bharat Biotech has signed an agreement to supply Brazil with the vaccine, and is applying to conduct trials in Bangladesh, Reuters reported. Bharat Biotech also signed an agreement with biopharmaceutical company Ocugen to develop its vaccine for the US market.
India has traditionally been receptive to vaccines, and there isn’t a strong anti-vaccination movement in the country, but Jesani, from the Indian Journal of Medical Ethics, says that could change if the government doesn’t act to restore confidence in Covaxin. Bhan, the bioethics expert, said an audit of the Bhopal trial would build confidence in the process.
If these initial questions linger and manifest as general anti-vaccination sentiment, that could be a problem for the public’s willingness not only to get the Covaxin vaccine, but also other coronavirus vaccines as India continues to report more than 10,000 cases each day.
Jesani said that is why it is so crucial that authorities investigate claims that some Bhopal participants didn’t know they were part of a trial.
“We don’t want people to lose faith. We don’t want people to lose trust in the vaccination,” he said. “If they lose trust in the Covid vaccine, they will lose trust in other vaccines.”
Esha Mitra reported from New Delhi and Bhopal, India. Julia Hollingsworth reported and wrote from Hong Kong. Additional reporting: Anup Dutta Photos and video: Ajay Bedi Graphics: Natalie Leung Editors: Hilary Whiteman and Jenni Marsh
Members of the Tshwane Special Infectious Unit on COVID-19 pick up a patient Jan. 15 in Pretoria, South Africa. (Gallo Images / Getty Images)
New data showing that two COVID-19 vaccines are far less effective in South Africa than in other places they were tested have heightened fears that the coronavirus is quickly finding ways to elude the world’s most powerful tools to contain it.
The U.S. company Novavax reported this week that although its vaccine was nearly 90% effective in clinical trials conducted in Britain, the figure fell to 49% in South Africa — and that nearly all the infections the company analyzed in South Africa involved the B.1.351 variant that emerged there late last year and has spread to the United States and at least 30 other countries.
Johnson & Johnson announced Friday that its new shot was 72% effective against preventing moderate or severe illness in the United States, compared with 66% in Latin America and 57% in South Africa.
Laboratory tests had suggested that the vaccines authorized in the U.S. — one from Pfizer and BioNTech, the other from Moderna and the National Institutes of Health — trigger a smaller immune response to the South Africa variant.
Now there is evidence from tests in people that some variants are less vulnerable to certain vaccines.
“From an evolutionary biology perspective, this is totally expected and anticipated,” said Dr. Michael Mina, a Harvard epidemiologist. “But it never feels good to be validated on something so scary.”
Researchers once believed it would take several more months, or even years, for the virus to develop resistance to vaccines. They said the speedy evolution is largely a result of the virus’ unchecked spread.
More than 100 million people have been infected worldwide, and each of those infections is an opportunity for the virus to randomly mutate.
A mutation that happens to give the virus an advantage — the ability to resist the body’s natural defenses, for example — can become the basis for a heartier variant.
One early sign that this process was underway was the significant number of people who were contracting the coronavirus a second time. It appeared that the training their immune systems received during the first infection was failing to protect them from new versions of the virus.
Scientists at Moderna and Pfizer-BioNTech worried that the same thing could happen with immunity induced by their vaccines. In laboratories, they took several versions of the virus and exposed them to blood samples from a small number of people who had been vaccinated.
The neutralizing antibodies produced in response to Moderna’s vaccine were equally effective against the original coronavirus and the B.1.1.7 strain that emerged in the United Kingdom but were far less effective against the South Africa strain. Pfizer’s vaccine was only slightly less effective against the South Africa variant compared with the others.
Experts had cautioned that laboratory tests were an imperfect model for understanding the immune response in people.
Other parts of the immune system, such as T-cells, might play a role in fighting a variant, even when neutralizing antibodies fall short, said Marc Lipsitch, a Harvard epidemiologist.
That’s why the Novavax trial — the first to test the interactions between variants and vaccines in the real world — was so concerning.
“Whether people who have been vaccinated get infected with the variant — that’s the real proof in the pudding,” said Dr. Otto Yang, an infectious-disease researcher at UCLA.
Novavax cautioned that its South Africa study, which included about 4,400 patients, was too small to offer a precise measurement on the vaccine’s efficacy.
The Johnson & Johnson results provided further evidence that the problem was serious.
Experts said the weaker performance of the vaccine in South Africa — where it was tested on about 6,500 people — almost certainly was a result of the predominance of the variant circulating widely there. Researchers believe that it is more contagious than other variants and that it has become more common in South Africa and elsewhere since the trial began in September.
Researchers said variants were also likely to blame for the subpar showing of the Johnson & Johnson vaccine in Latin America — where it was tested in more than 17,000 people in Argentina, Brazil, Chile, Colombia, Mexico and Peru.
The mutations of greatest concern are on the spike protein on the surface of the virus, because the current crop of vaccines train the immune system to recognize that protein. Mutations there increase the likelihood that the virus will slip by undetected.
Mina, the Harvard epidemiologist, likened the process to searching for a criminal by memorizing the appearance of only his nose and mouth. At first, this may prove sufficient. But if the criminal gets a nose job, investigators will wish they learned about his eyes, ears and hair as well.
Mina said a more diverse arsenal of vaccines, employing a variety of approaches, is needed.
In the meantime, Moderna has announced efforts to develop a booster shot to add to its current two-shot regimen in order to fend off the South Africa variant. The company also plans to test whether a third shot of the original formula could help with other strains.
BioNTech, the company that worked with Pfizer on its shot, is also considering developing an adjusted vaccine.
The United States reported its first known cases of the South Africa variant Thursday, in two people in South Carolina. The U.K. strain, which is also thought to be more contagious, is also circulating here.
In a briefing for reporters Friday, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, said the confirmation that more transmissible strains are now in the U.S. is a “wake-up call” that underscores the need to rapidly vaccinate Americans.
“Vaccinating as many people as we can, as quickly as we can” is the key to slowing the ability of the virus to mutate, he said. “Viruses cannot mutate if they cannot replicate.”
The U.S. is vaccinating an average of 1.2 million people a day, said Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention.
Experts say that is far too slow, because there’s no knowing what kind of advanced variants will exist by the time the vaccination campaign reaches critical mass.
They stress that vaccination must be accompanied by defensive tactics such as masking and social distancing until case numbers are negligibly low.
“If you think you’re going to simply vaccinate your way out of this, it’s going to be like whack-a-mole,” said Susan Butler-Wu, director of clinical microbiology at L.A. County-USC Medical Center.
An effective vaccination campaign must eventually stretch around the world. If an impressive strain were to pop up next year in, for example, Brazil, even a fully vaccinated U.S. could be in danger.
“You can vaccinate the hell out of America,” said Mina, but “until everyone is protected, we’re all still at risk.”
Fauci called for bolstering the government’s ability to detect new viral mutations. Genetic sequencing efforts have been fragmented, relying on academics and other groups to voluntarily upload their findings. The U.S. sequences just 1% of the millions of positive samples collected during routine coronavirus testing.
“We’re shining a flashlight around in the dark, hoping we spot dangerous variants,” said Anne Rimoin, an epidemiologist at UCLA. “What we really need to do is flip on the lights.”
This story originally appeared in Los Angeles Times.
People on a low-fat, plant-based diet ate fewer daily calories but had higher insulin and blood glucose levels, compared to when they ate a low-carbohydrate, animal-based diet, according to a small but highly controlled study at the National Institutes of Health. Led by researchers at the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the study compared the effects of the two diets on calorie intake, hormone levels, body weight, and more. The findings, published today (January 21, 2021) in Nature Medicine, broaden understanding of how restricting dietary carbohydrates or fats may impact health.
“High-fat foods have been thought to result in excess calorie intake because they have many calories per bite. Alternatively, high-carb foods can cause large swings in blood glucose and insulin that may increase hunger and lead to overeating,” said NIDDK Senior Investigator Kevin Hall, Ph.D., the study’s lead author. “Our study was designed to determine whether high-carb or high-fat diets result in greater calorie intake.”
The researchers housed 20 adults without diabetes for four continuous weeks in the NIH Clinical Center’s Metabolic Clinical Research Unit. The participants, 11 men and nine women, received either a plant-based, low-fat diet or an animal-based, low-carbohydrate diet for two weeks, immediately followed by two weeks on the alternate diet. The low-fat diet was high in carbohydrates. The low-carbohydrate diet was high in fats. Both diets were minimally processed and had equivalent amounts of non-starchy vegetables. The participants were given three meals a day, plus snacks, and could eat as much as desired.
Examples of dinners given to study participants: low-carb, animal-based diet (left) and low-fat, plant-based diet (right). Credit: Amber Courville and Paule Joseph, NIH
The main results showed that people on the low-fat diet ate 550 to 700 fewer calories per day than when they ate the low-carb diet. Despite the large differences in calorie intake, participants reported no differences in hunger, enjoyment of meals, or fullness between the two diets. Participants lost weight on both diets, but only the low-fat diet led to a significant loss of body fat.
“Despite eating food with an abundance of high glycemic carbohydrates that resulted in pronounced swings in blood glucose and insulin, people eating the plant-based, low-fat diet showed a significant reduction in calorie intake and loss of body fat, which challenges the idea that high-carb diets per se lead people to overeat. On the other hand, the animal-based, low-carb diet did not result in weight gain despite being high in fat,” said Hall.
These findings suggest that the factors that result in overeating and weight gain are more complex than the amount of carbs or fat in one’s diet. For example, Hall’s laboratory showed in 2019 that a diet high in ultra-processed food led to overeating and weight gain in comparison to a minimally processed diet matched for carbs and fat.
The plant-based, low-fat diet contained 10.3% fat and 75.2% carbohydrate, while the animal-based, low-carb diet was 10% carbohydrate and 75.8% fat. Both diets contained about 14% protein and were matched for total calories presented to the subjects, although the low-carb diet had twice as many calories per gram of food than the low-fat diet. On the low-fat menu, dinner might consist of a baked sweet potato, chickpeas, broccoli and oranges, while a low-carb dinner might be beef stir fry with cauliflower rice. Subjects could eat what and however much they chose of the meals they were given.
“Interestingly, our findings suggest benefits to both diets, at least in the short-term. While the low-fat, plant-based diet helps curb appetite, the animal-based, low-carb diet resulted in lower and more steady insulin and glucose levels,” Hall said. “We don’t yet know if these differences would be sustained over the long term.”
The researchers note that the study was not designed to make diet recommendations for weight loss, and results may have been different if participants were actively trying to lose weight. Further, all meals were prepared and provided for participants in an inpatient setting, which may make results difficult to repeat outside the lab, where factors such as food costs, food availability, and meal preparation constraints can make adherence to diets challenging. The tightly controlled clinical environment, however, ensured objective measurement of food intake and accuracy of data.
“To help us achieve good nutrition, rigorous science is critical − and of particular importance now, in light of the COVID-19 pandemic, as we aim to identify strategies to help us stay healthy,” said NIDDK Director Griffin P. Rodgers, M.D. “This study brings us closer to answering long-sought questions about how what we eat affects our health.”
Reference: “Effect of a plant-based, low-fat diet versus an animal-based, ketogenic diet on ad libitum energy intake” by Kevin D. Hall, Juen Guo, Amber B. Courville, James Boring, Robert Brychta, Kong Y. Chen, Valerie Darcey, Ciaran G. Forde, Ahmed M. Gharib, Isabelle Gallagher, Rebecca Howard, Paule V. Joseph, Lauren Milley, Ronald Ouwerkerk, Klaudia Raisinger, Irene Rozga, Alex Schick, Michael Stagliano, Stephan Torres, Mary Walter, Peter Walter, Shanna Yang and Stephanie T. Chung, 21 January 2021, Nature Medicine. DOI: 10.1038/s41591-020-01209-1
The research was supported by the NIDDK Intramural Research Program. Additional NIH support came from the National Institute of Nursing Research under grant 1Z1ANR000035-01.