- SARS-CoV-2 mRNA vaccines decouple anti-viral immunity from humoral autoimmunity Nature.com
- ACE2: its diverse functions, relationship with SARS-CoV-2, and the implications for COVID-19 disease sequelae News-Medical.Net
- Antivirals for adult patients hospitalised with SARS-CoV-2 infection: a randomised, phase II/III, multicentre, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn trial The Lancet
- Pharmacological disruption of mSWI/SNF complex activity restricts SARS-CoV-2 infection Nature.com
- Evaluating SARS-CoV-2 bivalent booster vaccine against severe COVID-19 outcomes News-Medical.Net
- View Full Coverage on Google News
Tag Archives: antiviral
Why Some People Never Become Infected With COVID-19
With the ongoing surge of COVID-19 infections in China, many are shocked by its scale and worried about a potential new wave hitting the rest of the world.
How can you better protect yourself if another wave does come to your region? Here, we take a close look into the factors impacting our antiviral immunity.
Some People Never Get Infected by Viruses
Looking at pandemics throughout history, one cannot ignore the impacts of the Black Death, which swept through Europe and reduced the population in some areas by more than half. Yet some people never got sick.
Cholera almost wiped out Europe, but some people stayed uninfected even though they ate the same contaminated food and drank the same cholera-tainted water.
Some doctors and nurses dedicated their lives to the leprous tribes, and yet they never had leprosy in their lives.
Two human challenge trials were done during the 1918 Spanish flu by two independent groups of doctors in Boston and San Francisco with 62 and 50 healthy volunteers, respectively.
Regardless of how many aggressive means were taken to try to infect people (even dropping mucus or bodily fluids from flu patients into the healthy volunteers’ eyes, noses, or throats), none of the participants became infected.

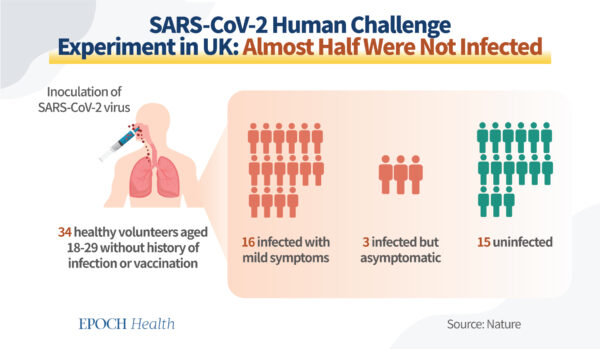
During the COVID-19 pandemic, a SARS-CoV-2 human challenge study published in Nature in 2022 found that out of the 36 healthy volunteers inoculated with the SARS-CoV-2 virus intranasally, only a little over half became infected with mild symptoms, and the other half were uninfected. Two were excluded from the per-protocol analysis, so the experiment went on with 34 participants.
This experiment goes to show that some people just don’t get infected.
Viruses ‘See’ People With Weakened Immunity
While people may look similar on the outside, we look very different in the microscopic world of viruses. Our immune systems look different, too.
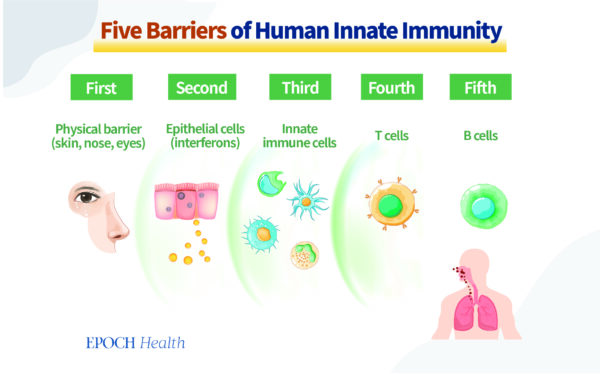
The immune system we were both with is sophisticatedly designed, layer upon layer, and acts like an army protecting us against various viruses and bacteria 24/7.
Viruses need suitable cells to replicate.
If a person’s cells are in a good antiviral state, there is no soil for the virus to spread its roots, so to speak, so that person won’t become infected.

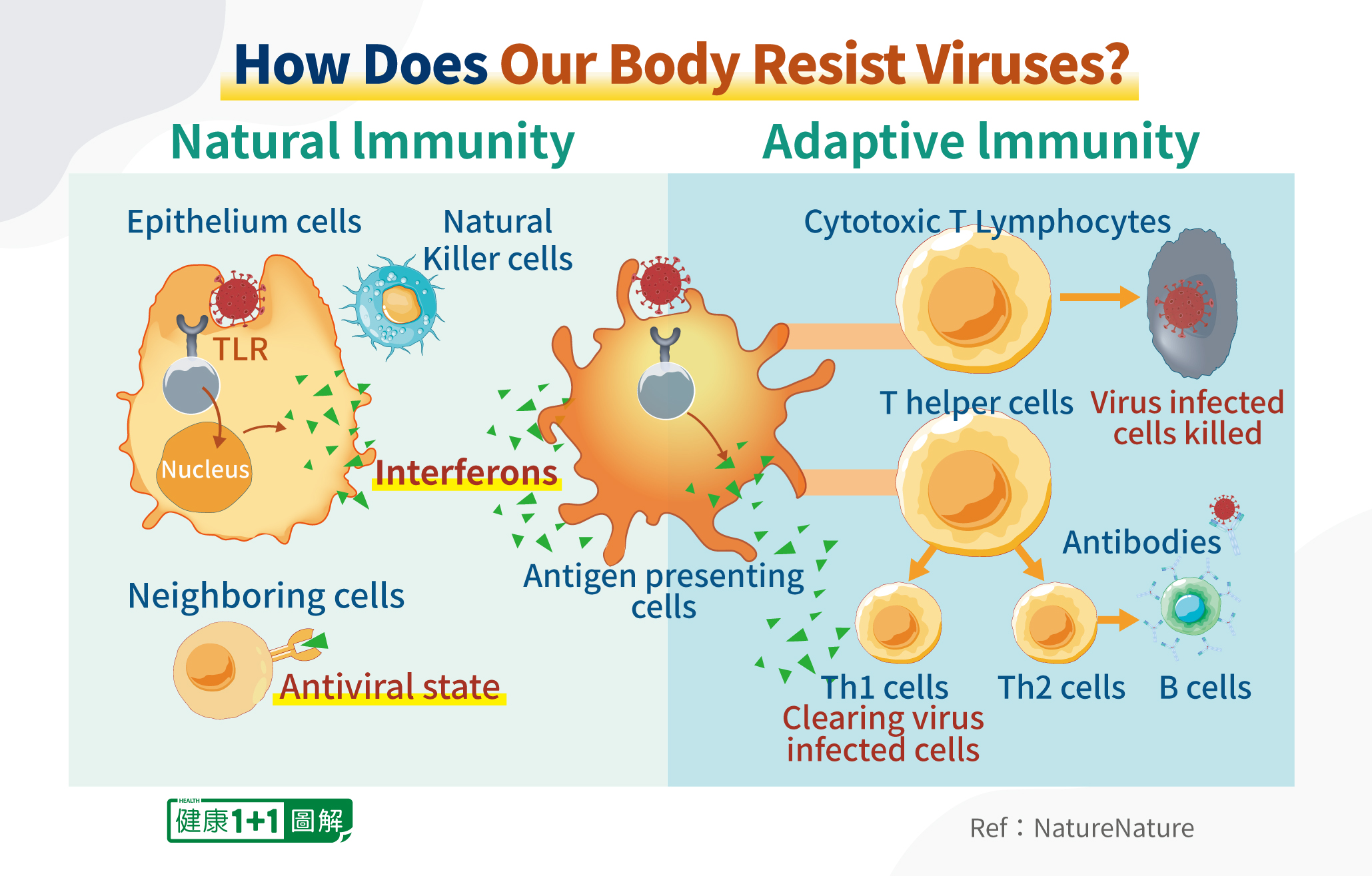
For instance, mucosal epithelial cells in our nose can automatically secrete a substance that puts this cell into an antiviral state.

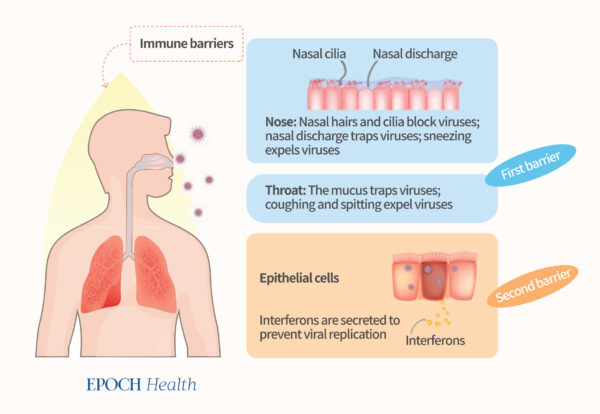
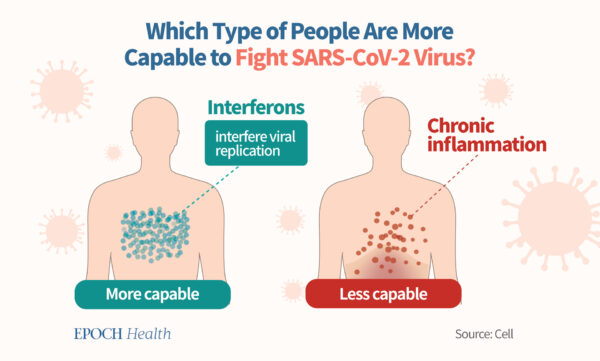
This substance is called interferon. It interferes with the replication of the virus, breaking down its protein, enzymes, and RNA so that the virus cannot survive in these cells.

Going deeper, there are a variety of immune cells, such as natural killer (NK) cells, macrophages, and lymphocytes. Each cell is like a special soldier possessing special skills to fight viruses.

Even if you become infected, if your immune system is strong, you will only be infected with mild disease, and you can quickly recover.
Research published in the journal Scientific Reports of Nature proves that at the early stage of infection, the more interferon is present, the lower the incidence of developing severe symptoms of COVID.
On the contrary, if a person has poor antiviral immunity, the virus will more likely to go wild in his or her body.
Two States of Immunity
There are generally two distinct states of immunity.
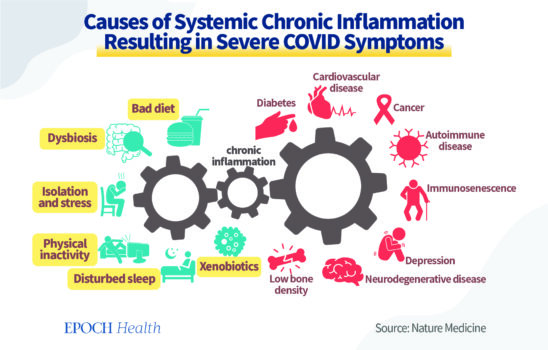
One is the antiviral state. It is characterized by strong antiviral immunity of the immune cells that can secrete interferons to eradicate viruses. The other is the systemic chronic inflammation state. This state makes people susceptible to viral infections.

A study published in Nature Medicine summarizes the causes of chronic inflammation and its consequences.

Having Purpose Promotes Antiviral Immunity
When we talk about strengthening immunity, people often think about improving nutrition or developing antibodies.
Those factors are important; boosting nutrition and adding exercise to one’s regimen will certainly help. At the same time, there are other internal ways to enhance our ability to fight viruses.
Everyone has emotions, thoughts, characteristics, and different mental states. People think that our thoughts are intangible, but they do in fact have material applications. Science has proved this point already.
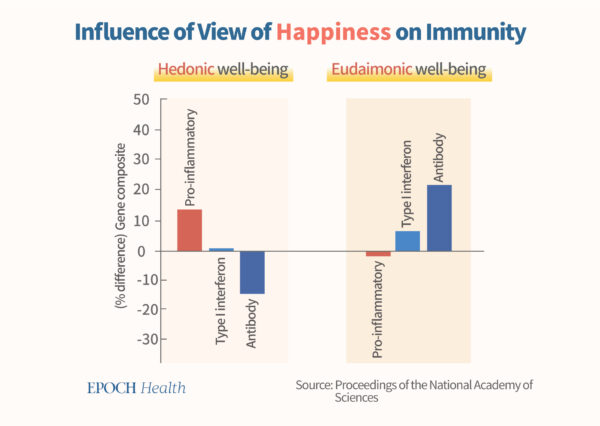
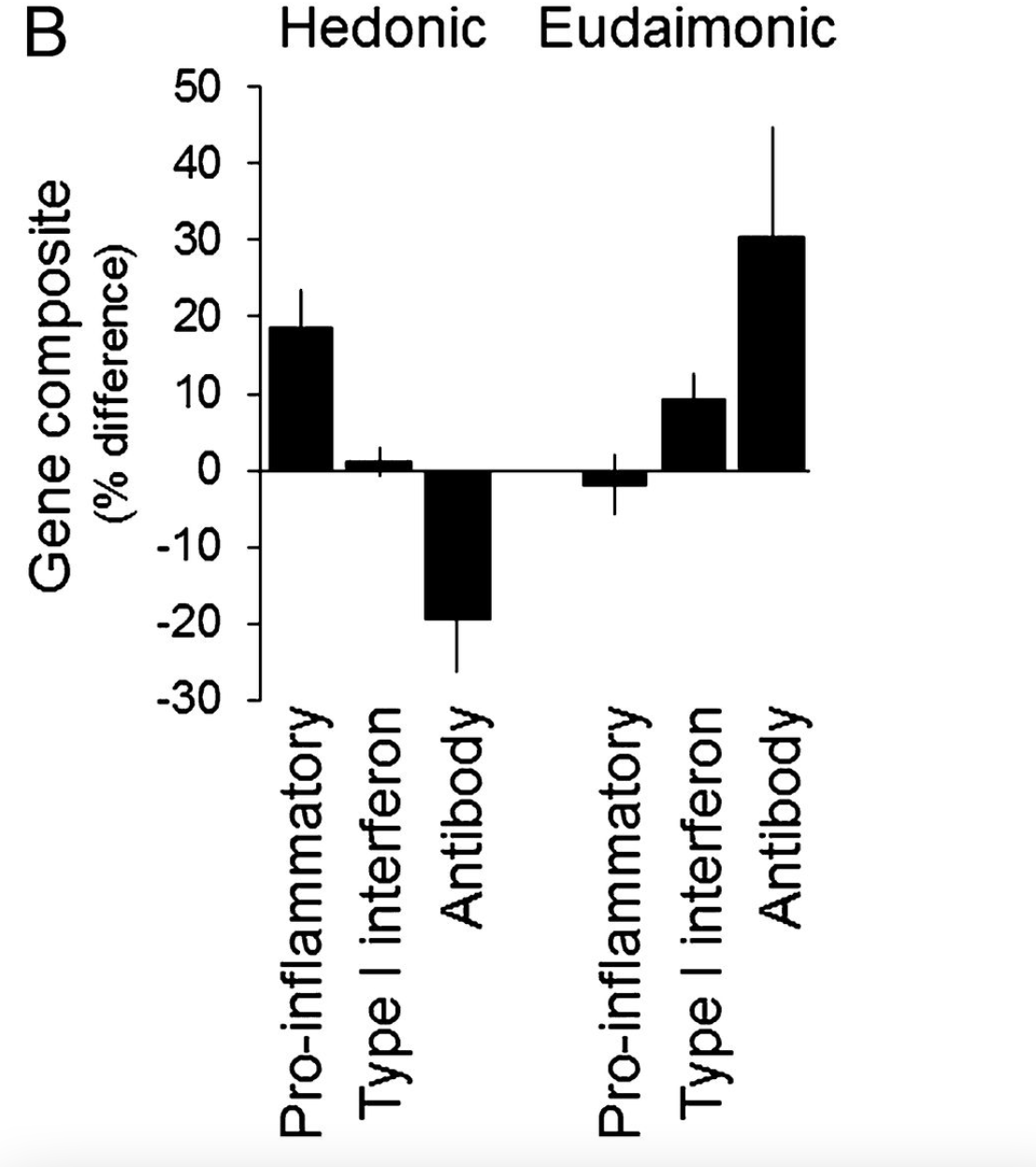
In psychology, there are two sorts of concepts regarding happiness: hedonic and eudaimonic. Hedonic refers to the happiness gained through pleasurable experience, and eudaimonic refers to happiness that comes from achieving purpose and meaning. A 2013 study published in a top-ranked journal discovered that people who were inclined to pursue justice and noble goals (eudaimonic) had higher interferon gene expression, higher ability to produce antibodies, and significantly lower expression of chronic inflammatory genes.

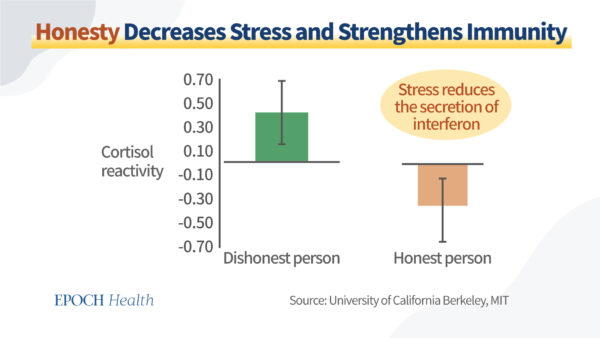
Furthermore, according to a Harvard University and University of California, Berkeley, study published in Current Opinion in Psychology in 2015 (pdf), people with honest hearts are less prone to viral infections. This is because the cortisol responsiveness of liars is significantly higher than that of truth-tellers. And the higher the cortisol responsiveness, the easier it is for the stress hormone levels in the body to rise.
Corticosteroids and cortisol have an inhibitory effect on immune cells and suppress the body’s ability to fight viruses. Therefore, dishonest behavior will lead to a decline in antiviral ability.
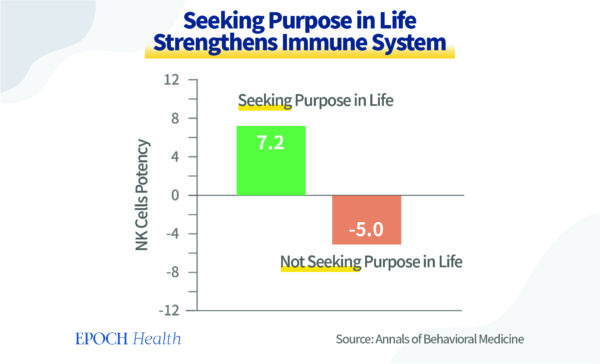
Additionally, research has found that people who seek purpose in life have stronger natural killer cell function and immunity.

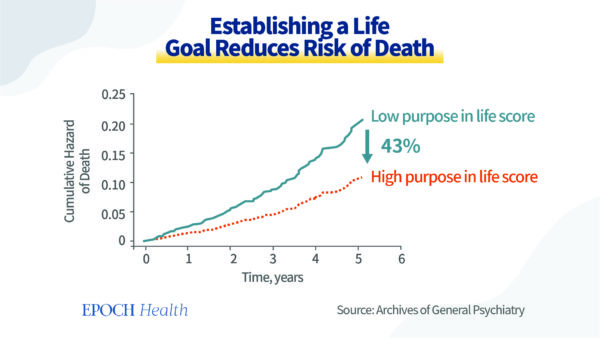
A study was conducted by the Rush Alzheimer’s Disease Center in the Departments of Behavioral Sciences and Neurological Sciences at the Rush University Medical Center in Chicago on the important determinant of health outcomes and mortality in community-dwelling elderly persons in the United States.
Researchers found that having a stronger sense of purpose in life effectively prevents lethal events. A person with a high score on the purpose in life measure had a 43 percent reduced risk of mortality compared to a person with a low score. Thus, developing and refining people’s sense of purpose can protect health and potentially save lives.
The scientific evidence supports that our thoughts, mindsets, and moral standards can affect the genes and functions of immune cells, affect hormone levels, and impact holistic antiviral immunity.
As a whole, our thoughts can contribute to whether or not we are infected in an epidemic, or whether or not we will be seriously ill after we are infected.
In traditional cultures, people who are kind, altruistic, honest, and who have a calm heart and humble attitude are normally healthier. Now we understand that it is because they produce high levels of interferon, strong NK cell function, and strong antiviral immunity. Such people are less susceptible to viral infections.
People with these qualities usually have a stable mind and better mental health and do not easily become anxious, depressed, or have negative and intense emotions.
I have a friend who has faith, is kind, often volunteers to help others, and has been in the COVID ward every day throughout the pandemic. This friend has never been infected with COVID-19. I also have many other friends similar to her who have remained uninfected during the pandemic, too.
Throughout the recent COVID surge in China, there have been an unusual number of high-profile Chinese officials who have died of suspected COVID-19 infections. As high-ranking officials in China, they enjoy state-of-the-art medical care and have adequately supplied first-class food, nutrients, and dietary supplements. So why have they been dying during this wave?
We all know about the fake news and falsification in China, including the cover-up and concealment of COVID-19 data, the suppression of whistleblowers, and the suppression of people who dare to speak the truth.
The high-ranking officials in China—not all, but many of them—did not speak the truth to the people. They either executed the cover-up or helped with the cover-up. From a biological perspective, their bodies’ stress hormone levels may be much higher than people who do not bear the stress of dishonesty. If they lived in that state constantly, the chronically elevated stress hormones would have done great damage to their immunity.
These officials do not put the well-being of the Chinese people before profits or power. Therefore, the interferon gene expression level of their immune cells is expected to be lower than that of people who care for others.
If these officials were to have had more virtuous minds and kinder hearts, they might have been less prone to viral infections or at risk for severe disease.
There is a Chinese traditional saying: “Illnesses are caused by 70 percent mental and 30 percent physical.” During the pandemic, it’s not only important to keep a good physical state, but to also keep a kind and virtuous mindset to aid your immune system.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.


Dr. Yuhong Dong, a medical doctor who also holds a doctorate in infectious diseases in China, is the chief scientific officer and co-founder of a Swiss biotech company and former senior medical scientific expert for antiviral drug development at Novartis Pharma in Switzerland.
Some people are experiencing ‘Paxlovid rebound’ after taking the COVID antiviral pill. Here’s what you should know.

When the antiviral medication Paxlovid was approved in 2021 to treat COVID-19, doctors began noticing a perplexing trend among some of the patients who took the medication: a rebound case of the virus. After treatment, some people would recover and test negative for the virus, only to test positive or have symptoms come back a few days later. “Paxlovid rebound,” as it’s known, received a lot of media attention when President Biden, first lady Jill Biden, as well as Drs. Anthony Fauci and Rochelle Walensky, director of the Centers for Disease Control and Prevention, all experienced it last year after taking the medication.
Scientists are not sure why this rebound effect occurs when taking Paxlovid, but here are a few things we do know.
What is Paxlovid? How does it work?
Paxlovid is an oral antiviral pill that can be prescribed to people who come down with COVID-19 and are at risk for developing severe disease. This can be individuals who are unvaccinated, the elderly or people with other medical conditions, such as cancer or diabetes. The drug, developed by Pfizer, can protect these high-risk patients from needing hospitalization. Those who are vaccinated but who are at risk for severe outcomes of COVID-19 can also benefit from taking Paxlovid.
U.S. regulators granted emergency use authorization for Paxlovid in December 2021. Today the drug is available by prescription only, from a physician or pharmacist. Anyone ages 12 and older who weighs at least 88 pounds and who is at high risk for severe disease is eligible for the medication. Patients with severe kidney disease — or who are on dialysis — or people with severe liver disease, however, should not take Paxlovid. The drug can also interact with other medications such as those that treat high cholesterol, high blood pressure and migraines, so patients taking these drugs should avoid taking Paxlovid.
Like many antivirals, Paxlovid works best when taken early in the course of illness. The CDC recommends treatment begin within the first five days of experiencing symptoms. Once a person is prescribed the medication, they will take three Paxlovid pills twice a day for five days for a full course that adds up to 30 pills.
The antiviral therapy consists of a combination of two oral antiviral drugs — nirmatrelvir and ritonavir — which work together to stop the viral replication process. By reducing a person’s viral load, the medication lessens the severity of their symptoms.
In clinical trials, which were conducted when the Delta variant was predominant, Paxlovid was found to reduce the risk of hospitalization or death by 89% in high-risk people. Since its approval, many clinical studies that have been conducted around the world have also confirmed the drug’s high level of protection against hospitalization and death.
With Omicron being a highly immune-evasive variant that has rendered many antibody treatments ineffective, vaccine experts worried that Paxlovid would lose its effectiveness too. Fortunately, that doesn’t seem to be the case. According to recent research, the drug continues to offer significant protection against hospitalization and death and can also offer a substantial benefit even to vaccinated patients diagnosed with COVID-19.
Other studies, however, have found no evidence of Paxlovid benefiting people younger than age 65.
“I don’t think we need to push Paxlovid in every 20-year-old who comes down with COVID or 35-year-old who’s healthy,” Dr. Bruce Farber, chief of public health and epidemiology at Northwell Health, the largest health care system in New York state, told Yahoo News. “But in those who are at high risk, those who are elderly, who have not been vaccinated, those who have comorbidities, those who are immunosuppressed, [for] those people [it] can make a significant difference,” he added.
In addition to keeping high-risk patients from getting very sick, Paxlovid can reduce the risk of symptoms of long COVID, a November study conducted by the Department of Veterans Affairs found.
What is Paxlovid rebound?
The CDC defines Paxlovid rebound as when, after completing the full five-day course of treatment, a person experiences either a reemergence of symptoms or tests positive after having tested negative for COVID-19. According to the CDC, this rebound effect tends to occur between two and eight days after initial recovery. But experiencing a rebound, the agency said, doesn’t mean that a person was resistant to Paxlovid, nor does it mean they were reinfected with the virus. Additionally, the CDC has said Paxlovid rebound cases are typically mild, resolve within a few days, and there’s no evidence that additional treatments are needed for these patients.
Despite Paxlovid’s efficacy even in the setting of Omicron, the medication is being underutilized in the U.S. and other parts of the world. According to a report by the London-based health analytics firm Airfinity, U.S. physicians have prescribed the drug in only about 13% of new COVID-19 cases, Nature recently reported. Experts have said concerns about suffering from potential Paxlovid rebound is one of the reasons this may be happening.
Farber also said that another reason Paxlovid is being underutilized has to do with the virus itself.
“This virus is much less virulent even though it’s more contagious,” he said, adding that the need for Paxlovid “became less.”
Scientists are still studying why this rebound effect occurs when taking Paxlovid, as well as who is more likely to experience it. However, recent research has found that rebound can also happen to people who develop COVID-19 and don’t take Paxlovid. Studies are underway to understand why this happens, Farber said.
“More recent data suggests that rebound also occurs in people who recover from COVID who have not gotten Paxlovid, and it occurs at probably similar rates, whether you take Paxlovid or not,” Farber said, adding that rebound cases after taking the drug were initially thought to occur in roughly 5% of cases but that research has shown it may happen more often than initially thought. “More recent articles say it may be as common as 10 or 15% of cases,” he said.
What to do if you experience Paxlovid rebound
If someone’s symptoms return or they test positive after Paxlovid treatment, the CDC advises following its isolation guidance and quarantining again for five days. Isolation can end after this period if a person is fever-free for 24 hours without the use of fever-reducing medications. The agency also recommends wearing a mask for 10 days after rebound symptoms start.
The CDC encourages doctors and patients to report Paxlovid rebound cases to Pfizer’s portal for adverse events associated with the drug.
Finally, Farber said that Paxlovid rebound is still fairly uncommon and that it shouldn’t deter people and their doctors from using the life-saving medication when needed.
“In theory, it could prolong their isolation. But I think [people] should realize that this can occur even without Paxlovid. So it becomes really not an important distinguisher, of whether they get it or not,” he said.
Beijing to distribute Pfizer antiviral drug as Covid wave overwhelms health system
Beijing
CNN
—
Beijing will begin distributing Pfizer’s Covid-19 drug Paxlovid to the city’s community health centers in the coming days, state media reported Monday.
The report comes as the city grapples with an unprecedented wave of infections that has severely strained its hospitals and emptied pharmacy shelves.
The state-run China News Service reported Monday that after receiving training, community doctors will administer the medicine to Covid-19 patients and give instructions on how to use them.
“We have received the notice from officials, but it is not clear when the drugs will arrive,” it cited a worker at a local community health center in Beijing’s Xicheng district as saying.
Paxlovid remains the only foreign medicine to treat Covid that has been approved by China’s regulator for nationwide use, but access is extremely difficult to come by. When a Chinese healthcare platform offered the antiviral drug earlier this month, it sold out within hours.
Azvudine, an oral medicine developed by China’s Genuine Biotech, has also been approved.
After nearly three years of lockdowns, quarantines and mass testing, China abruptly abandoned its zero-Covid policy this month following nationwide protests over its heavy economic and social toll.
The abrupt change in policy has sparked panic buying of fever and cold medicines, leading to widespread shortages, both at pharmacies and on online shopping platforms. Long lines have become routine outside fever clinics and hospital wards overflowing with patients in the capital Beijing and elsewhere in the country.
On Monday, Chinese state media CCTV quoted President Xi Jinping as saying the country needed a more targeted health strategy to protect people’s lives as the Covid situation in China changes.
“Xi Jinping emphasized that our country is currently facing a new Covid outbreak situation and new responsibilities, we need to conduct our patriotic health movement in a more targeted manner,” the CCTV report said.
It was one of the first public statements made by Xi about China’s Covid situation since the government’s decision to ease its strict restrictions.
An emergency room doctor in Beijing told the state-run People’s Daily on Thursday that four doctors on his shift did not have time to eat or drink. “We have been seeing patients nonstop,” he said.
Another emergency room doctor told the newspaper he had been working despite having developed fever symptoms. “The number of patients is high, and with fewer medical staff, the pressure is multiplied,” said the doctor.
In a sign of the strain on Beijing’s medical system, hundreds of health professionals from across China have traveled to the city to assist medical centers.
As the capital, Beijing has some of the best medical resources in the country. However, the abrupt zero-Covid u-turn has left people and health facilities ill-prepared to deal with a surge in infections.
China’s official Covid case count has become meaningless after it rolled back mass testing and allowed residents to use antigen tests and isolate at home. It has stopped reporting asymptomatic cases, conceding it was no longer possible to track the actual number of infections.
According to an internal estimate from the National Health Commission, almost 250 million people in China have caught Covid in the first 20 days of December – accounting for roughly 18% of the country’s population.
Experts have warned that as people in big cities return to their hometowns for the Lunar New Year next month, the virus could sweep through China’s vast rural areas, where vaccination rates are lower and medical resources are severely lacking.
Hope for long Covid sufferers as Pfizer antiviral for patients left with lingering symptoms trialed
Hope for long Covid sufferers as new study will trial Pfizer’s antiviral Paxlovid in patients left with lingering symptoms months later
- 100 people who have had long Covid symptoms for 3+ months will take Paxlovid
- Researchers want to see if it will help with brain fog, fatigue and weakness
- 1 in 13 US adults suffer with long Covid, and trial results are expected next year
Paxlovid – an antiviral made by Pfizer – is now being looked at as a possible long Covid treatment.
The pharma giant’s flagship Covid drug gained emergency approval in the US last December to treat high-risk patients – slashing their risk of death by 90 per cent.
It is currently the only medication you can take at home to treat Covid and has been given to millions of vulnerable Americans with underlying health conditions.
Now, researchers at Stanford are about to launch the first clinical trial of the drug to see it may also provide relief to people who are still ill months and years after clearing the virus.
Prior research has indicated that people given the drug are a quarter less likely to suffer long Covid – which most commonly causes intense tiredness, brain fog and muscle weakness.
As of yet, there are no proven treatments for long Covid, and no one knows what causes the ongoing symptoms.
A popular theory is that there may be bits of leftover virus wreaking havoc in the body. A recent study suggested people with long Covid suffer physical alterations to their brain months after clearing the initial infection.
More than 15million Americans are officially estimated to have long Covid to varying degrees.


Trial participants will take the antiviral drug for ten days longer than people usually take it for, to see if it needs longer to work
The new study hopes to sign up 200 adults who have been negative for Covid for three months yet still suffer symptoms.
Half the participants will receive Paxlovid and half will take a placebo.
To treat an infection, Paxlovid is given as six pills a day for five days, but participants in the new study will take the drug for 15 days to test the theory that the drug needs more time to have its full effect.
Results of the trial are expected next year.
The first participant in the trial was 67-year-old Bill Fimbres from California, who has been suffering with long Covid symptoms for a year-and-a-half, including a loss of smell and taste, debilitating fatigue and brain fog.
He said: ‘It’s like you have somebody else’s brain.’
Mr Fimbres will take his first dose of either the drug or placebo on Monday.
He told NBC News: ‘If I could get rid of just one of my symptoms, that would be great. I’m just going on hope.’
Evidence indicating Paxlovid might stunt long-term symptoms already exists.
A study by the Department of Veterans Affairs this month suggested those who received the drug immediately after their Covid diagnosis were 26 per cent less likely than those who did not take the antiviral to have lasting symptoms three months on.
However, the participants were all aged 60 or above with additional health issues, meaning the findings may not be applicable to everyone.
Long Covid has puzzled scientists and physicians since it first popped on their radar in 2020.
Its causes have not been figured out, but experts believe it could be tied to the body’s immune response to the virus.
There have also been previously known cases of people suffering long-term symptoms after suffering more common viruses like the flu.
The CDC estimates that around 7.5 per cent of American adults are suffering from long Covid symptoms.
Sufferers are generally under the age of 50, and are more likely to be women. Reports of long Covid are most common in southern states like Kentucky and Alabama.
Bay Area COVID patients flag ‘Paxlovid rebound’ after taking antiviral treatment
When Berkeley resident Myriam Misrach tested positive for the coronavirus last month, she started taking the COVID antiviral pill Paxlovid the same day. Over the five-day course of treatment, her cough and shortness of breath mostly faded, but a couple days after taking the final pill, her symptoms came roaring back.
For 48 hours thereafter, she also had a fever, headache, nausea, runny nose and lost her sense of taste, she said. And she once again tested positive for the virus — despite having tested negative and feeling much better just a few days prior.
“I had everything in the book,” said Misrach, 66, who is vaccinated and boosted. “It was not at all a mild case.”
Misrach continued testing positive for two weeks after that and today is still coughing, though the other symptoms have subsided. What was even more puzzling, she said, was that her husband had also just taken Paxlovid and for him, it “worked beautifully” — he started feeling better almost immediately and stayed that way, though he too tested positive after initially testing negative.
“I’m not blaming Paxlovid but I think they need to study it more,” she said.
As the number of Americans taking the Pfizer drug skyrockets, many people are reporting similar “rebound” after taking the drug — including some vaccine scientists and doctors who’ve documented their experiences on Twitter. In addition to a recurrence of symptoms, rebound also means that someone who thought they’d recovered might still be infectious and should isolate for additional days.
All known cases of Paxlovid viral rebound appear to have been resolved without patients needing hospitalization, say doctors who prescribe the drug and researchers who are studying the issue. They overwhelmingly agree that this does not give them pause about prescribing the antiviral medication, which in clinical trials reduced the risk of COVID hospitalization and death by nearly 90%. They say if someone is eligible for Paxlovid, the patient should still get it, despite the potential of experiencing rebound symptoms, because it’s living up to its promise by indeed keeping people out of the hospital.
Rebound, also known as relapse, isn’t uncommon in infectious diseases. Doctors often see it in patients who took antibiotics or antivirals, where the infection returns after the treatment is completed because the virus or pathogen wasn’t cmpletely cleared, said Dr. Prasanna Jagannathan, a Stanford immunologist and infectious disease physician.
The Paxlovid rebound phenomenon is an example of what happens when a new medication — probably the most closely watched drug in recent memory, second only to COVID vaccines — starts to get used widely in the real world and elicits outcomes that may not have been observed during clinical trials at such high levels. This doesn’t mean the drug is failing, scientists and doctors noted, but rather that it needs to be studied further and that its dosage or duration of usage may need to be tweaked.
It’s not clear why rebound is happening, or how often it occurs in the real world. In Pfizer’s clinical trials, it occurred in 2% of the people who took Paxlovid. Many doctors who prescribe the antiviral say they hear about rebound anecdotally from patients, and that it appears to be more common than it was in trials. But that could be in part because of reporting bias, where the people who experience rebound are more likely to report it than those who didn’t have the issue.
“We’ve all heard anecdotes of patients we’ve taken care of that experience this, so it’s clearly a phenomenon,” said Jagannathan, who has prescribed Paxlovid to 25 to 30 patients and observed rebound in two of them. “What that true number is, no one knows yet.”
Pfizer and the U.S. Food and Drug Administration are tracking rebound cases for further study. Providers and patients can report cases to Pfizer’s and the FDA’s respective adverse event reporting systems.
Researchers are eyeing a few potential explanations for viral rebound.
One small study, which has not yet been peer reviewed, suggests the issue is probably not drug resistance due to viral mutation or a problem with a patient’s immune response. Rather, patients may not have been exposed to Paxlovid enough. This could mean that instead of the five-day course currently authorized by the FDA, people may need to take the drug for longer, or at a different dosage. The study, which was posted on a pre-print site this week, looked at three vaccinated and boosted adults who took Paxlovid, including one who experienced rebound. That person was infected with the BA.2 omicron subvariant.
Patients and health care providers can report instances of suspected Paxlovid rebound to Pfizer and the U.S. Food and Drug Administration, which are tracking the phenomenon for further study.
To report it to Pfizer, go to Pfizer’s COVID-19 Treatment Adverse Event Reporting website and submit a form online.
To report it to the FDA, go to FDA MedWatch and submit a form online or by fax at 1-800-332-0178. Call 1-800-332-1088 for questions.
“Our hypothesis or best guess at this point is we think there’s insufficient drug exposure to get rid of the virus,” said the study’s lead author, UC San Diego’s Dr. Aaron Carlin, who studies emerging and reemerging viral infections and how they interact with the immune system. “There’s likely going to be studies to see if people need 10 days instead of five days to try to prevent that rebound from occurring.”
Another small study, initially posted in late April and updated last week by the VA Boston Health System, also suggests the reason for relapse isn’t because the virus mutated after patients took Paxlovid. The authors said further research is needed to determine the cause of relapse.
Pfizer’s Paxlovid trials were done in vaccinated and unvaccinated people when delta and earlier variants were circulating. Now, it’s people infected with omicron and omicron subvariants who are taking the drug, including many who are vaccinated. So it’s possible their immune systems are responding to the drug a little differently, which might help explain rebound. It could also be that omicron and its subvariants lead to a longer period of viral shedding than delta, so people may now need a longer course than five days.
The UC San Diego study analyzed several coronavirus variants and their sensitivity to Paxlovid, and didn’t find significant differences in how they responded to the drug. But there is some evidence suggesting that the neutralizing antibody response in vaccinated people is lower against omicron than delta, “so there may be something about omicron and the immune system that contributes to this (rebound), but we don’t understand that yet,” Carlin said.
If it turns out the virus does become resistant to Paxlovid in the future, it may be that combining it with other antivirals may help. Treating HIV with a single drug almost immediately leads to drug resistance, but treating it with three drugs doesn’t, Carlin said.
“It’s a warning, but I don’t think it’s a reason people should not take the drug,” Carlin said. “It’s still highly effective. We just have to understand whether it can be used in a way to make it even better to avoid the rebound.”
Catherine Ho (she/her) is a San Francisco Chronicle staff writer. Email: cho@sfchronicle.com Twitter: @Cat_Ho
Is Paxlovid, the Covid Pill, Reaching Those Who Most Need It?
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
As the nation largely abandons mask mandates, physical distancing, and other covid-19 prevention strategies, elected officials and health departments alike are now championing antiviral pills. But the federal government isn’t saying how many people have received these potentially lifesaving drugs or whether they’re being distributed equitably.
Pfizer’s Paxlovid pill, along with Merck’s molnupiravir, are aimed at preventing vulnerable patients with mild or moderate covid from becoming sicker or dying. More than 300 Americans still die from covid every day.
National supply counts, which the Biden administration has shared sporadically, aren’t the only data local health officials need to ensure their residents can access the treatments. Recent federal changes designed to let large pharmacy chains like CVS and Walgreens efficiently manage their supplies have had an unintended consequence: Now many public health workers are unable to see how many doses have been shipped to their communities or used. And they can’t tell whether the most vulnerable residents are filling prescriptions as often as their wealthier neighbors.
KHN has repeatedly asked Health and Human Services officials to share more detailed covid therapeutic data and to explain how it calculates utilization rates, but they have not shared even the total number of people who have gotten Paxlovid.
So far, the most detailed accounting has come from the drugmakers themselves. Pfizer CEO Albert Bourla reported on a recent earnings call that an estimated 79,000 people received Paxlovid during the week that ended April 22, up from 8,000 a week two months earlier.
Unlike covid vaccinations or cases, HHS doesn’t track the race, ethnicity, age, or neighborhood of people getting treatments. Vaccination numbers, initially published by a handful of states, allowed KHN to reveal stark racial disparities just weeks into the rollout. Federal data showed that Black, Native, and Hispanic Americans have died at higher rates than non-Hispanic white Americans.
Los Angeles County’s Department of Public Health has worked to ensure its 10 million residents, especially the most vulnerable, have access to treatment. When Paxlovid supply was limited in the winter, officials there made sure that pharmacies in hard-hit communities were well stocked, according to Dr. Seira Kurian, a regional health officer in the department. In April, the county launched its own telehealth service to assess residents for treatment free of charge, a model that avoids many of the hurdles that make treatment at for-profit pharmacy-based clinics difficult for uninsured, rural, or disabled patients to use.
But without federal data, they don’t know how many county residents have gotten the pills.
Real-time data would show whether a neighborhood is filling prescriptions as expected during a surge, or which communities public health workers should target for educational campaigns. Without access to the federal systems, Los Angeles County, which serves more residents than the health departments of 40 entire states, has to use the limited public inventory data that HHS publishes.
That dataset contains only a slice of information and in some cases shows months-old information. And because the data excludes certain types of providers, such as nursing homes and Veterans Health Administration facilities, county officials can’t tell if patients there have taken the pills.
Because so little data is available, Kurian’s team created its own survey, asking providers to report the ZIP codes of patients who have received the covid therapies. With the survey, it’s now easier to figure out which pharmacies and clinics need more supplies.
But not everyone completes it, she said: “Oftentimes, we have to still do some guesstimating.”
In Atlanta, staff at Good Samaritan Health Center would use detailed information to direct low-income patients to pharmacies with Paxlovid. Though the drug wasn’t readily available during the first omicron surge, the next one will be “a new frontier,” said Breanna Lathrop, the center’s chief operating officer.
Ideally, she said, her staff would be able to see “everything you need to know in one spot” — including which pharmacies have the pills in stock, when they’re open, and whether they offer home delivery. Student volunteers built the center a similar database for covid testing earlier in the pandemic.
Paxlovid and molnupiravir became available in the U.S. in late December. They have quickly become the go-to treatments for non-hospitalized patients, replacing nearly all the monoclonal antibody infusions, which are less effective against current covid strains.
Though the government doesn’t record Paxlovid use by race and ethnicity, researchers tracked those trends for the first-generation infusions.
Amy Feehan, co-author of a CDC-funded study and a clinical research scientist at Ochsner Health in Louisiana, found that Black and Hispanic patients with covid were significantly less likely than white and non-Hispanic patients to receive those initial outpatient treatments. Other researchers found that language difficulties, lack of transportation, and not knowing the treatments existed all contributed to the disparities. Feehan’s study, using data from 41 medical systems, found no large discrepancies for hospitalized patients, who didn’t have to seek out the drugs themselves.
Patients at Atlanta’s Good Samaritan Health Center often don’t know that if they get tested quickly they can receive treatment, Lathrop said. Some assume they don’t qualify or can’t afford it. Others wonder if the pills work or are safe. There are “just a lot of questions in people’s minds,” Lathrop said, about whether “it benefits them.”
When Dr. Jeffrey Klausner was a deputy officer at the San Francisco Department of Public Health, “our first priority was transparency and data sharing,” he said. “It’s important to build trust, and to engage with the community.” Now a professor at the University of Southern California, he said federal and state officials should share the data they have and also collect detailed information about patients receiving treatment — race, ethnicity, age, illness severity — so that they can correct for any inequities.
Public health officials and researchers who spoke with KHN said that HHS officials may not think the data is accurate or have adequate staff to analyze it. The head of HHS’ therapeutics distribution effort, Dr. Derek Eisnor, suggested as much during an April 27 meeting with state and local health officials. One local official asked the federal agency to share local numbers so they could increase outreach in communities with low usage. Eisnor responded that because HHS doesn’t require providers to say how much they use, the reporting “is kind of mediocre at best,” adding that he didn’t think it was his agency’s role to share that information.
Eisnor also said that state health departments should now be able to see local orders and usage from pharmacy chains like CVS, and that the agency hopes to soon release weekly national data online. But counties like Los Angeles — which has requested access to the federal systems with no success — still don’t have access to the data they need to focus outreach efforts or spot emerging disparities.
Spokesperson Tim Granholm said that HHS is looking into ways to share additional data with the public.
Recordings of the weekly meetings, in which HHS officials share updates about distribution plans and answer questions from public health workers, pharmacists, and clinicians, were posted online until March. HHS’ media office has since repeatedly declined to grant KHN access, saying “the recordings are not open to press.” That’s because HHS wants to encourage open conversation during the meetings, according to Granholm. He did not say what legal authority allows the department to bar media from the public meetings. KHN obtained the public records through Freedom of Information Act requests.
A senior White House official said that the Biden administration is attempting to collect accurate data on how many people receive Paxlovid and other treatments but said it doesn’t define success by how many people do so. Its focus, the official said, is on making sure the public knows treatments are available and that doctors and other providers understand which patients are eligible for them.
We still need to know where the pills are going, Feehan said. “We need that data as soon as humanly possible.”
Until then, Los Angeles County’s Kurian and her peers will keep “guesstimating” where residents need more help. “If someone can just give us a report that has that information,” she said, “of course, that makes it easier.”
Why Some People Won’t Get Infected, Even After Covid Exposure
Recently an unprecedented study was conducted in the UK; a Covid-19 “Human Challenge Trial.” In it, 36 unvaccinated young adults were recruited to be injected with the coronavirus SARS-CoV-2 through the nose.
While the ethics of this study are undoubtedly questionable, the results were even more surprising. None of these people got seriously sick, and, more importantly, only half of these people exposed to the virus were infected.
The study raised an important question: Why didn’t everyone get sick? Even though the virus was injected directly into their noses, some weren’t infected.
For answers, we turned to Dr. Yuhong Dong, an expert in infectious diseases and antiviral drug development.
“We may think it’s incredible, but in the real world, we’re often exposed to an environment with the same virus concentration where some people get infected and some don’t,” Dr. Dong said. “What’s the reason? The study was designed to answer the question of why some people are resistant to viral infection.”
“People are probably just as curious as to how the tests were done. Everyone must be very concerned about the safety of the subjects upon hearing of this,” she said.
Dr. Dong notes that in the UK study, participants were infected with a strain that was not Omicron or as harsh as Delta. The study used an earlier pre-Alpha strain, which still had considerable pathogenicity.
So only a very healthy group of people, aged 18–29 years old, were considered as eligible subjects. And the study was designed very rigorously to ensure their safety.
The Infection Period

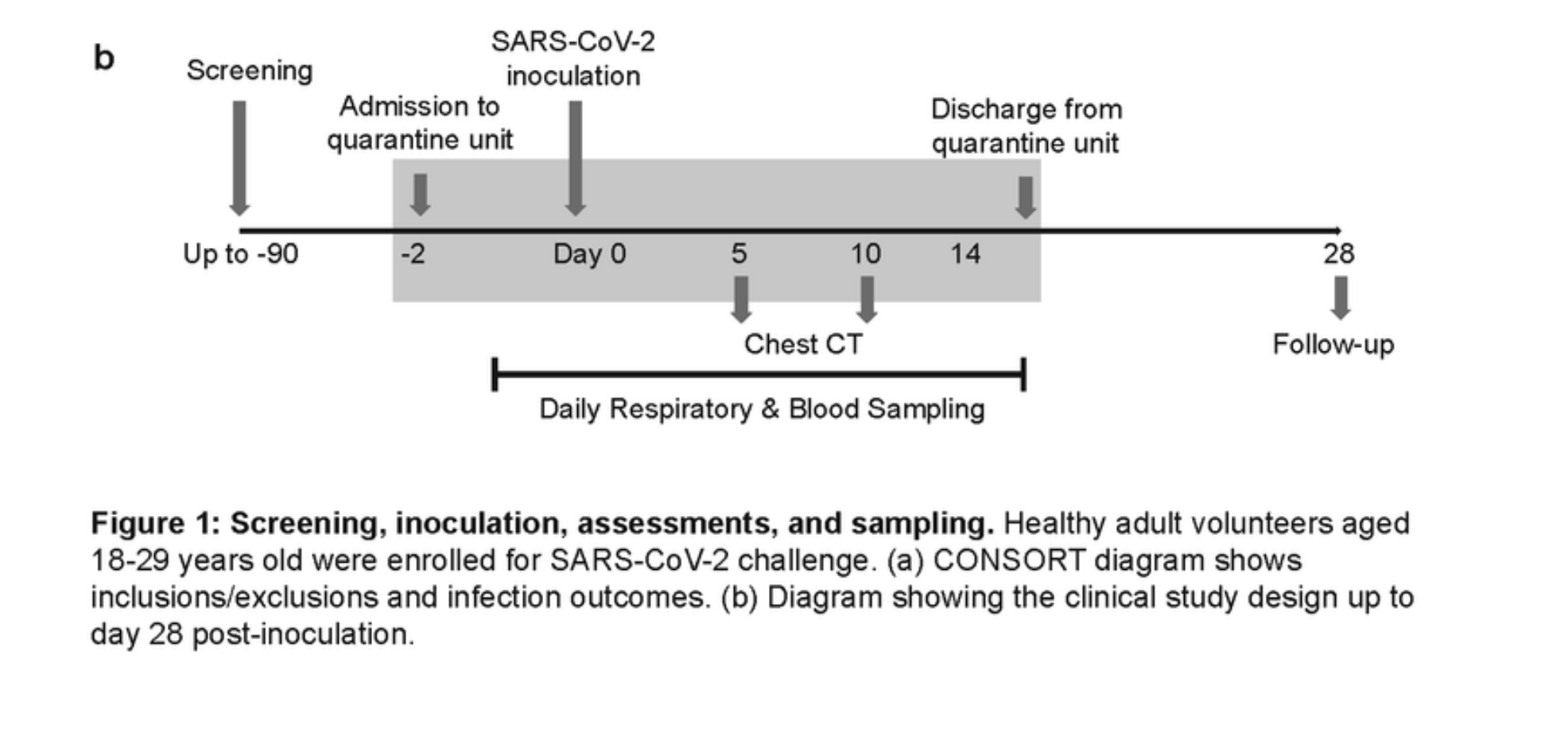
After 14 days of inoculating SARS-CoV-2 into the nose, the results can be put into three categories:
The first category were the 17 people who had no infection at all. There were no symptoms, no virus detected in the throat or the nose, and no antibodies in the blood. “The excellent natural immunity of these people won the battle against the virus without even breaking a sweat,” Dr. Dong said.
The second category were the asymptomatic patients—no symptoms, no virus was detected in the throat, but there were antibodies in the bloodstream—this means that asymptomatic immune reactions have happened in these people. Their immunity can still be considered to be quite good.
The third category were the 18 subjects who were symptomatic. The virus as well as antibodies were present in their bloodstream. The levels of inflammatory proteins in their bloodstream also increased. In the end, the infection was eradicated at the cost of countless immune cells like macrophages. Their natural immunity is rather weak when compared with the two previous categories, Dr. Dong explained, so their adaptive immunity (like a team of Navy SEALS) had to intervene, which resulted in antibodies.
What Was Different About Those Who Weren’t Infected?
The entire group of 36 participants was made up of healthy young adults, so it wasn’t as if those infected had pre-existing conditions. Then, what was different about the 17 who weren’t infected?
“We have to look at how the human body fights viruses,” Dr. Dong said.
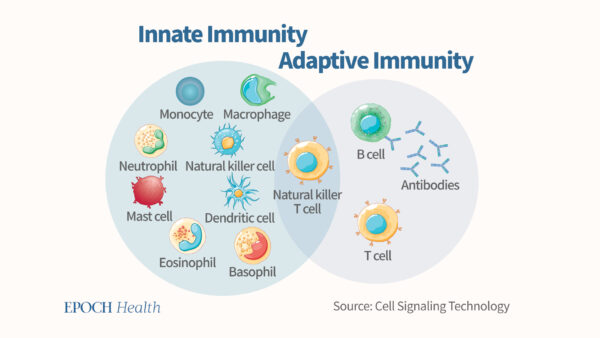
“The immune system is like a well-established, compartmentalized military force, with each division performing their own duties and cooperating in combat. It is divided into the innate immune system and acquired immune system. The innate immune system responds quickly and protects us no matter what is attacking the body.”
“This map basically shows the key cells in the immune system, including mucosal epithelial cells, phagocytes, macrophages, T cells, B cells, Natural killers, etc..”

In people who are not infected, high levels of protective antibodies are not detected in the blood, indicating that the virus has not really entered the blood.
“In the mucosal epithelium stage, most of them are likely to be blocked. This is the human body’s first resistance against incoming viruses. For those with multiple immune barriers, when the specific immune system is online, it is often so because the virus has broken through the mucosal immunity and activated the acquired immunity, like the third group, indicating that the mucosal immunity is relatively weak and is not enough to resist the strength of the virus.
Resisting the Virus: Antiviral State and Interferon Activation
“How does the immune system help swing the fight around? A very important factor in winning is the state of the immune system before the battle, where the body is deploying its troops, is critical. Is the human immune system in a good state?
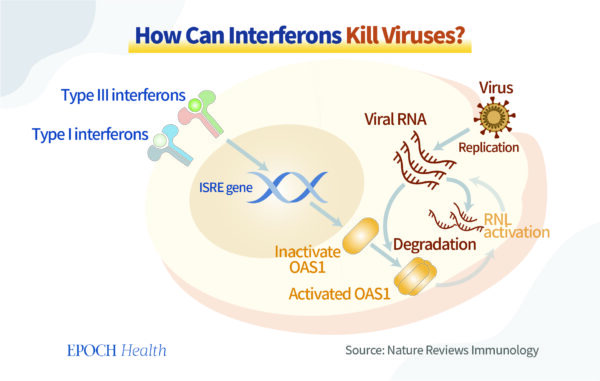
“The role of the interferon is very important. It is like a marker that adjusts the human body to a state where viruses can hardly replicate,” Dr. Dong said.
“When something like a FBI facial recognition system is functioning and detecting viral particles in the cells, multiple intracellular mechanisms will be activated to increase the large production of interferons by those infected cells. Interferons are the natural enemy of viruses. Why? It interferes with virus replication at every step of its life cycle, e.g. prohibiting DNA transcription, degrading mRNA, inhibiting translation from mRNA to protein and viral packaging.”
The first batch of infected cells will release interferons to neighboring cells, helping them become resistant to viral invasion.
“The human body can function like a switch, turning interferon production on and off. If it’s on, then interferon levels are healthy and the body is strong against viruses. How do we ensure our front line epithelium cells have a healthy level of interferons? During the course of this pandemic, there has been a lot of discussion of the role of B cells, antibodies, and now more recently, T cells. But why haven’t we talked about interferons?
“People pay more attention to the part of acquired immunity, vaccines, monoclonal antibodies and the like. Vital components of the body’s natural immune system are often overlooked. However, this part of the natural immune system remains to be an irreplaceable component of our immune system.
If the adaptive immunity (T cells, B cells) were already activated, it means that the viruses have already broken through the first line of defense in the superficial mucosal layer to the deeper blood or tissue layer. This means that we are already infected by the virus, similar to those 18 subjects who were infected by SARS-CoV-2 .
That is the real reason why current COVID-19 intramuscular vaccines can’t protect us from infection, as the antibodies induced by vaccines are working in the background, but not at the front line.
Think about two countries: in the first country your regular men in blue (or natural immunity cells) are able to keep the whole country safe. In the second country you see the military (adaptive immunity cells) patrolling the streets all day. Which country seems to be safer? Obviously, the first one.
“Therefore, the key is to be mentally prepared for an incoming infection by taking care of the body during times of ‘peace’ and to not fight unprepared battles. If you go to war when the virus has already arrived, and think about how to prevent the virus from coming, you’re already a step too late. Early preventive efforts long prevail directly dealing with the virus.”
Immunity and Inflammation
Then, under what circumstances would someone lack antiviral immunity?
“A large number of scientific studies have also found that people who suffer from chronic diseases and chronic inflammation have a higher risk of being infected with viruses, or developing severe symptoms. Chronic inflammation itself is an abnormal state of the body, because the body is “in” “flame,” or the body is on fire—a state of war.
Dr. Dong explained that severe COVID-19 patients often have cytokine storms, which is caused by excessive secretion of inflammatory cytokines. This situation is like adding fuel to the fire.
“In order to fight the virus, we must first put out the fire, that of our own body’s inflammation first. If your own body is already “on fire,” and you have an incoming virus, then you’re going to overload your body. It can’t handle something that puts this much strain on it, and will make any infection much more severe. As a result, a lot of your own tissues and cells will be damaged, perhaps beyond repair.
“As mentioned earlier, if people are healthy and there are plenty of interferons, our switch is “on” and antiviral; if there is chronic inflammation inside the body and we don’t have a lot of interferons, then our switch is “off” and we’d be easily infected with.
The ‘Antiviral State’
The most important thing is how to help people enter an antiviral state, where the body is ready for any incoming infections.
Various factors involving people’s daily life, sleep schedules, diet (alcohol consumption), stress level, etc. all contribute to this.
There are over a dozen lifestyle factors, Dr. Dong said, but many people watch out for a few.
For example, when it comes to bolstering the immune system, vitamin supplements, and looking at nutrition is easy for everyone to understand, because the effects can be seen through a microscope.
But when it comes to regulating emotions, relieving stress, and changing what we’re conscious about, people feel it is too out of touch to be relevant.
However, scientists’ research has proved that our thoughts and mindset can affect how well our immune cells function.
For example, as mentioned in many previous interviews with Dr. Dong, people with two different views of happiness—hedonic and altruistic—express different levels of interferons by our immune cells. Therefore, although our mindset is intangible, it still objectively exists and can even affect the state of our immune cells.

“The mind cannot be seen under the microscope, but the microscope is just a tool we use. Tools are man-made; today with a microscope, you can see molecules, and tomorrow it may be an atomic microscope, or even a super microscope, and you can see smaller things.
“Therefore, the fundamental reason why these people are not infected with the coronavirus is that at the macroscopic level, the body’s immune system—spleen, bone marrow, lymph nodes and other organs or tissues—function normally.
“At the molecular level, it’s about immune cells, related molecules (interferons, etc) and other substances. But at a more microscopic level, there may be more manifestations, which we cannot “see” yet.
“Although invisible, these manifestations could exist, and can very much affect the tangible things.
“Therefore, to really study the science of our human body, we can’t just stick to the molecular or cellular level, but go a little deeper. Think mindset, spirit and so on. In the UK Human Challenge Trial, the deeper reason why some people weren’t infected with the virus may also be related to substances at a more microscopic level. It would be great if the study designers collected information about the subjects’ vitamin D levels, alcohol consumption, sleeping schedule, stress level, as well as their views on well-being, etc.”
Also, we have to remember that these Covid vaccines do not prevent viral infection. “It’s an inherent defect, a congenital defect, if you will, of the design concept of these vaccines,” Dr. Dong said. “The role of the vaccine is very similar to B cells, which are producing antibodies, and it is not on the front line of infection, so it is not surprising that it cannot prevent infection.
What the Vaccine Is Missing
Specific immunity depends on the viral gene sequence, so vaccines are locked to a specific generation of a virus. Because of this, newer covid generations such as Omicron can “evade” the vaccine. The vaccine also has an “expiration date.” This is because the vaccine is a foreign substance, and eventually gets metabolized in the body. The antibodies induced by the vaccine are metabolized as well. The vaccine alone is not very reliable.
In the end, you should keep in mind that the current COVID vaccine doesn’t prevent an infection in the first place. This is true for any virus and any variant.
Therefore, if we want to find something that can overcome these defects and really prevent infection, we need something else..
So what “shot” should we get? Our God-given natural immunity is fighting against all variants of any viruses or bacteria at the front line of the battlefield all the time. Isn’t this a great “vaccine”? It’s a pity that not everyone is aware of what it’s capable of, or understands how to maintain it, but totally gets that you should get premium gas every once in a while.
However, the antibodies induced by Covid vaccines could help an infected person neutralize invading viruses in the bloodstream, which could reduce the disease severity for those people with weakened natural immunity. This is the reason why Covid vaccines could protect in cases of symptomatic Covid infections, reducing severe disease or deaths. So vaccinations in general could in that way help reduce the burden of medical resources and bring benefits for human society.
Signs of the Body
In these 18 subjects, the virus first appeared in the throat in just under two days. It is interesting to note that the virus was only detected in the nose 3 days after it was first injected. Dr. Dong explained that a trait of the virus, its ability to look for a habitable environment first before multiplying, was responsible for this. The throat, having a rich blood system, was a great match for the virus. Virus levels tended to peak in about five days.

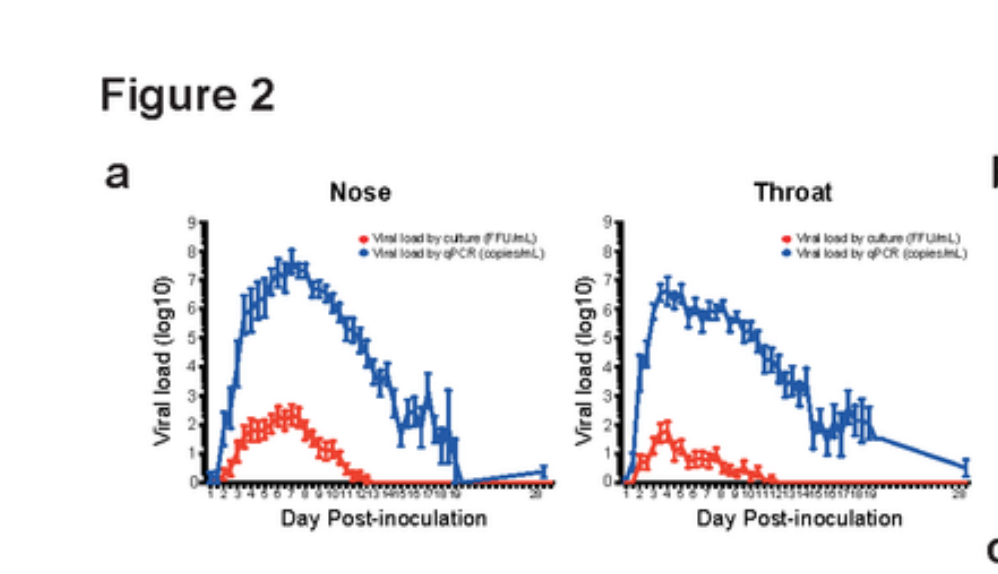
“But on the flip side, the throat, which seemed to be a suitable environment for the virus to multiply, is also better equipped with a defense system,” Dr. Dong said. “The throat is located behind the nasal cavity. The mucosal immune system, which also happens to be there, is relatively strong. For example, we have two tonsils in the back of the throat. The two tonsils are two strategically important goalkeepers in our body that fight against all sorts of pathogens as the very first line of defense.”
“Even in healthy people, the lymphocytes in the throat remain in a state of readiness. Once bacteria, viruses, and other pathogens invade, they will immediately retaliate. In the early stages of a common cold, symptoms such as a sore throat and phlegm will appear, which is the result of the ability of mucosal immunity to eliminate the virus or bacteria. As long as one’s immunity is strong enough, a common cold is not a big deal.
“However, if you suffer from a cold while having a relatively poor immune system, which can be caused by lack of sleep, long-term fatigue, stress, etc. even the time it takes to recover from a common cold can take several weeks to a few months. This is a clear sign for us to change our lifestyle and to treat our immune system a little better.”
Therefore, how much a cold affects us is actually more of a sign from our body, an indication of how well our immune system is doing. We should pay more attention to what our body is telling us.
References:
https://assets.researchsquare.com/files/rs-1121993/v1/2f0e9953-432e-4601-b98e-4ae5c08e025d.pdf?c=1644278080%EF%BC%9B2
Nutrition and immunity: lessons for COVID-19 | European Journal of Clinical Nutrition (nature.com)
Toll-like Receptors and Type I Interferons* – Journal of Biological Chemistry (jbc.org)
A functional genomic perspective on human well-being | PNAS
Chronic inflammation in the etiology of disease across the life span | Nature Medicine
Efficacy of Antiviral Agents against the SARS-CoV-2 Omicron Subvariant BA.2
To the Editor:
The omicron (B.1.1.529) variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is responsible for coronavirus disease 2019 (Covid-19), has spread rapidly around the world and has already become the predominant variant circulating in many countries. As of February 2022, omicron variants have been divided into four distinct sublineages: BA.1, BA.1.1, BA.2, and BA.3.1 Most circulating omicron variants belong to sublineage BA.1; however, in Denmark, India, and the Philippines, the sublineage BA.2 is now becoming dominant.2
As compared with the Wuhan/Hu-1/2019 reference strain, the sublineage BA.2 of the omicron variant has 16 amino acid substitutions in the receptor-binding domain of the spike (S) protein of SARS-CoV-2,2 which is the primary target for monoclonal antibody–based therapy. The BA.2 and BA.1 variants share 12 of these 16 substitutions; however, BA.2 has four substitutions in the receptor-binding domain (i.e., S371F, T376A, D405N, and R408S) that differ from those in BA.1. These findings suggest that there may be differences in the effectiveness of monoclonal antibodies against these different omicron sublineages.
Accordingly, we examined the neutralizing ability of therapeutic monoclonal antibodies that have been approved by the Food and Drug Administration, individually and in combination, against the omicron BA.2 subvariant hCoV-19/Japan/UT-NCD1288-2N/2022 (omicron/BA.2; NCD1288), which was isolated from a traveler who arrived in Japan from India. Whole-genome sequencing analysis of the NCD1288 virus stock confirmed that it had the 16 substitutions that are characteristic of the omicron variant in the receptor-binding domain of the S protein, as compared with the Wuhan/Hu-1/2019 reference strain (Table S1 in the Supplementary Appendix, available with the full text of this letter at NEJM.org).
Efficacy of Monoclonal Antibodies and Antiviral Drugs against the Omicron/BA.2 Subvariant in Vitro.
A live-virus focus reduction neutralization test (FRNT) showed that both LY-CoV016 (marketed as etesevimab) and LY-CoV555 (marketed as bamlanivimab), individually and in combination, lost neutralizing activity against omicron/BA.2 (NCD1288) (Table 1). These findings are similar to our previous findings with omicron/BA.1 (hCoV-19/Japan/NC928-2N/2021; NC928)3 and omicron/BA.1.1 (hCoV-19/Japan/NC929-1N/2021; NC929).4 BA.1.1, a subvariant of BA.1, has the R346K mutation in the S protein (Table S2). However, REGN10987 (marketed as imdevimab), which was previously shown to lose neutralizing activity against omicron/BA.1 (NC928) and omicron/BA.1.1 (NC929),3,4 had neutralizing activity against omicron/BA.2 (NCD1288).
In addition, the combination of REGN10987 and REGN10933 (marketed as casirivimab) also inhibited omicron/BA.2 but did not inhibit omicron/BA.1 or omicron/BA.1.1. However, the FRNT50 (the titer of monoclonal antibodies required for a 50% reduction in the number of infectious foci) value of this combination therapy was higher by a factor of 43.0 to 143.6 for omicron/BA.2 than for an ancestral strain — SARS-CoV-2/UT-NC002-1T/Human/2020/Tokyo (NC002) — and other variants of concern (i.e., the alpha [B.1.1.7], beta [B.1.351], gamma [P.1], and delta [B.1.617.2] variants).
REGN10933, COV2-2196 (marketed as tixagevimab), and COV2-2130 (marketed as cilgavimab) neutralized omicron/BA.2. The COV2-2196–COV2-2130 combination inhibited omicron/BA.2 with a low FRNT50 value (14.48 ng per milliliter); however, the FRNT50 values of this combination were higher by a factor of 1.4 to 8.1 for omicron/BA.2 than for the ancestral strain and other variants of concern.
S309 (the precursor of sotrovimab), which has been shown to have lower neutralizing activity against omicron/BA.1 and omicron/BA.1.1 than against the ancestral strain and other variants of concern,3,4 had even less neutralizing activity against omicron/BA.2 in our study. The FRNT50 value of this monoclonal antibody was higher by a factor of 12.2 to 49.7 for omicron/BA.2 than for the ancestral strain and other variants of concern.
The susceptibilities of omicron/BA.2 (NCD1288) to remdesivir, molnupiravir, and nirmatrelvir were similar to those of the ancestral strain and other variants of concern (i.e., 50% inhibitory concentration values for these three agents that differed by factors of 2.5 to 4.5, 0.7 to 1.6, and 1.5 to 3.3, respectively) (Table 1).3 Clinical studies are warranted to determine whether these antiviral therapies are indeed effective against omicron/BA.2 infections. Our data indicate that some therapeutic monoclonal antibodies (REGN10987–REGN10933, COV2-2196–COV2-2130, and S309) have lower neutralizing activity against omicron/BA.2 than against earlier variant strains.
Emi Takashita, Ph.D.
National Institute of Infectious Diseases, Tokyo, Japan
Noriko Kinoshita, M.D.
National Center for Global Health and Medicine, Tokyo, Japan
Seiya Yamayoshi, D.V.M., Ph.D.
Yuko Sakai-Tagawa, Ph.D.
University of Tokyo, Tokyo, Japan
Seiichiro Fujisaki, Ph.D.
National Institute of Infectious Diseases, Tokyo, Japan
Mutsumi Ito, D.V.M.
Kiyoko Iwatsuki-Horimoto, D.V.M., Ph.D.
University of Tokyo, Tokyo, Japan
Peter Halfmann, Ph.D.
University of Wisconsin–Madison, Madison, WI
Shinji Watanabe, D.V.M., Ph.D.
National Institute of Infectious Diseases, Tokyo, Japan
Kenji Maeda, M.D., Ph.D.
National Center for Global Health and Medicine, Tokyo, Japan
Masaki Imai, D.V.M., Ph.D.
University of Tokyo, Tokyo, Japan
Hiroaki Mitsuya, M.D., Ph.D.
Norio Ohmagari, M.D., Ph.D.
National Center for Global Health and Medicine, Tokyo, Japan
Makoto Takeda, M.D., Ph.D.
Hideki Hasegawa, M.D., Ph.D.
National Institute of Infectious Diseases, Tokyo, Japan
Yoshihiro Kawaoka, D.V.M., Ph.D.
University of Tokyo, Tokyo, Japan
[email protected]
Supported by grants from the Center for Research on Influenza Pathogenesis (HHSN272201400008C, to Dr. Kawaoka), and from the Center for Research on Influenza Pathogenesis and Transmission (75N93021C00014, to Dr. Kawaoka), funded by the National Institute of Allergy and Infectious Diseases, and by a Research Program on Emerging and Reemerging Infectious Diseases (JP20fk0108412 and JP21fk0108615, to Dr. Kawaoka; JP21fk0108104, to Dr. Watanabe), a Project Promoting Support for Drug Discovery (JP20nk0101632, to Dr. Kawaoka), the Japan Program for Infectious Diseases Research and Infrastructure (JP21wm0125002, to Dr. Kawaoka) from the Japan Agency for Medical Research and Development, and a Grant-in-Aid for Emerging and Reemerging Infectious Diseases from the Ministry of Health, Labor, and Welfare, Japan (20HA2007, to Dr. Hasegawa).
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
This letter was published on March 9, 2022, at NEJM.org.
Drs. Takashita, Kinoshita, and Yamayoshi contributed equally to this letter.
Japan’s Kowa says ivermectin showed ‘antiviral effect’ against Omicron in research
Test tube with Corona virus name label is seen in this illustration taken on January 29, 2020. REUTERS/Dado Ruvic
TOKYO, Jan 31 (Reuters) – Japanese trading and pharmaceutical company Kowa Co Ltd (7807.T) said on Monday anti-parasite drug ivermectin showed an “antiviral effect” against Omicron and other variants of coronavirus in joint non-clinical research.
Kowa did not provide further details. The firm has been working with Kitasato University, a medical university in Tokyo.
Clinical trials evaluating the drug, which is used to treat parasites in animals and humans, are ongoing but promotion of the drug as a COVID-19 treatment has generated controversy.
The drug is not approved for treatment of COVID-19 in Japan and the U.S. Federal Drug Administration has repeatedly warned against its use.
Register now for FREE unlimited access to Reuters.com
Register
Reporting by Sam Nussey and Rocky Swift;
Editing by Tomasz Janowski
Our Standards: The Thomson Reuters Trust Principles.