The concept of viral escape from antibody neutralization seems intimately familiar in our post-COVID world—it’s the reason that we wait in line for new iterations of vaccines while dreadingthe inevitable arrival of new viral variants which can evade those vaccines. It’s a stark reminder that as our immune systems, scientists, and governments fight this virus, the virus fights back. In a recent preprint posted to bioRxiv, Timothy Yu, a graduate student in the lab of Dr. Jesse Bloom, and colleagues report efforts to predict viral escape from complex mixtures of neutralizing antibodies. In doing so, they hope to leverage state-of-the-art experimental and computational techniques to stay ahead in the arms race between virus and man, while potentially gaining new insight into how antibody mixtures interact with viral antigens on a fundamental level.
First, some vocabulary: antibodies are small proteins produced by our immune system whose job it is to bind viral proteins called antigens (for example, the spike protein on the surface of SARS-CoV-2) and neutralize or prevent them from invading our cells. To get more specific, any given antibody only binds a specific portion of its corresponding antigen—this region is called an epitope. We would like to imagine a simple scenario, whereby a viral infection causes your body to produce a single antibody type targeting a specific epitope, which the virus will slowly mutate to disrupt antibody binding and escape neutralization. However—as is usually the case in biology—reality is more complicated. Viral infection or immunization causes your body to produce a mixture of antibodies which recognize many different epitopes. While this is thought to increase the durability of anti-viral responses, we know from experience that viruses are still able to escape from these ‘polyclonal’ mixtures of antibodies by accumulating mutations in multiple antigenic regions (multiple epitopes). Understanding how viruses manage this escape—and developing tools to predict when they will—is of prime public health and basic science importance.
Methods exist to experimentally test whether a viral variant can lead to escape from antibody mixtures, but they are relatively low-throughput and laborious, as each variant needs to be tested individually—a tall order in situations when viral adaptation is rapid, and many different variants arise in the population. Crucially, these methods also rely on prior knowledge of the mutations to produce, which leaves us constantly ‘one step behind’ the virus we are trying to fight.
In the evolutionary chess match between the coronavirus and humans, scientists’ next move can’t come soon enough for the millions of Americans relying on treatments known as monoclonal antibodies. These lab-made therapies are rapidly losing their healing power, forcing researchers around the world to devise new antibodies that are both more potent and more resistant to new variants.
Some monoclonal antibodies have been rendered largely ineffective as the virus has mutated; others are expected to become so this winter if a wave of new omicron subvariants comes to dominate the pandemic landscape. For instance, the U.S. Food and Drug Administration recently warned that the widely used therapies Bebtelovimab and Evusheld may no longer work against some versions of the coronavirus.
The development is especially worrisome for people with weakened immune systems; vaccines are less effective in these patients, and many have instead turned to antibody therapy for protection.As these treatments wane, millions of people are at an increased risk of getting covid-19.
“I would say it’s a big problem,” said Michael Barnett, associate professor of health policy and management at Harvard University’s T.H. Chan School of Public Health.
People with weakened immune systems represent about 3 percent of all Americans and 12 percent of U.S. patients hospitalized with covid-19. Moreover, one of the most effective alternative treatments remaining, Paxlovid, has interactions with other drugs that would make it too risky for use by people with compromised immune systems, especially organ transplant patients.
Driven by this urgent need, scientists are exploring new ways to tackle the problem — including antibodies that seek out fresh targets among the vulnerable parts of the virus.
“I would hope that some of these will be in clinical trials soon, and then it won’t take long” to determine whether they work, said William Haseltine, a former Harvard Medical School professor who founded the university’s cancer and HIV/AIDS research departments.
“Either it protects you from infection, or it doesn’t.”
One new antibody cocktail developed by the Sherbrooke, Quebec, biotechnology company Immune Biosolutions is in clinical trials in South Africa and Brazil. Participants receive the treatment as a mist sprayed into their mouths for about three minutes while they breathe normally.
“We saw a sharp decline in viral loads” during the Phase 1 safety testing, said Bruno Maranda, the company’s chief medical officer.
For its Phase 2 tests, the company is conducting two distinct trials to see whether the cocktail has the desired effects: one with patients who have mild to moderate covid-19, the other with patients hospitalized with severe covid-19.
Two of the three antibodies in the cocktail, known as IBO123, take aim at a familiar region of the spike protein where the virus attaches to a human cell. This region is an obvious place to block the virus, but scientists have discovered a drawback. The target changes frequently, allowing the virus to slip away from the roadblocks researchers put in its way.
“There is a huge immune pressure on the virus,” explained Andrés Finzi, an associate professor at the University of Montréal whose lab helped developed the antibody cocktail. So far, evolution has favored mutations that allow the spike protein to shake off antibodies that try to prevent it from grabbing onto our cells. These mutations have fueled the rise of the variants and subvariants that are defeating the current lab-made antibodies.
That’s why the third antibody in Immune Biosolutions’ cocktail attacks the opposite end of the protein, called the stem helix. This region is what allows viral and human cell membranes to fuse together during the infection process. The new antibody acts like a set of hands strangling the stem helix.
This section of the spike protein is in scientists’ crosshairs because it has stubbornly remained the same even as the virus has churned out new variants and subvariants. When a section of a protein resists change, it is a sign that it is important, even essential, in order for the protein to work.
If an antibody disrupts this rigid part of the virus, the pathogen is less likely to mutate its way around the attack.
So far, the third antibody has been effective in tests against all of the coronavirus variants and subvariants except for XBB, on which it has yet to be tested, Finzi said. Maranda said he expects to see results from their first Phase 2 trial by the end of the year. Organizers of the second trial are still recruiting patients with severe covid-19. A third trial testing the cocktail’s ability to prevent infection is scheduled to start in a few weeks.
Two other antibodies that zero in on stable portions of the spike protein were discovered in a lab at the Pasteur Institute in Paris and developed by the French biotechnology company Spiklmm. They have now entered Phase 1 clinical trials.
Hugo Mouquet, head of the Humoral Immunology Lab at the Pasteur Institute, said by email that the two new antibodies have been effective in a lab dish against all of the common coronavirus variants, though they have yet to be tested against the new omicron subvariants BQ.1, BQ.1.1 and XBB.
If approved for use, these antibodies would be given to people with weakened immune systems before they have been exposed to the coronavirus. Like the antibody cocktail Evusheld, they would be used to prevent infection. By contrast, Bebtelovimab is given to patients after infection but within seven days or less of displaying symptoms of covid-19.
In addition, a July paper in the journal Science described a pair of new antibodies that target another stable section of the coronavirus’ spike protein, the fusion peptide. This part of the spike “acts like a grappling hook and inserts into the human cell membrane, pulling the membrane closer to the virus membrane,” said Joshua Tan, chief of the Antibody Biology Unit at the National Institute of Allergy and Infectious Diseases.
Although lab-made antibodies that hit the fusion peptide and the stem helix are less potent, Tan said, they are effective against a broader array of coronaviruses. In the lab, Syrian hamsters treated with one of his team’s antibodies and then infected with the coronavirus suffered less severe disease and recovered more quickly than infected hamsters that received no treatment.
In a paper published more recently in the journal Cell Host & Microbe, Tan and his colleagues identified two more monoclonal antibodies that both attack the spike protein’s stem helix. In tests on infected hamsters, these antibodies helped the animals maintain weight. Infected hamsters that were not given either of the antibodies lost about 10 percent of their body weight within six days. The study interpreted weight loss as a measure of disease because sick hamsters tend to eat less.
Tan could not say when the monoclonal antibodies examined in these studies might proceed to clinical trials.
Bing Chen, a professor of pediatrics at Harvard University who has been investigating the atomic structure of the spike protein, said that so far antibodies directed againstthe virus’s binding site have remained more potent than those aimed at other sections of the protein. He also stressed that developing better monoclonal antibodies should not take priority over other medical tools.
“You need much more effective vaccines, for sure,” Chen said. While the vaccines were highly effective early on, viral mutations have allowed more so-called breakthrough infections in people who are fully vaccinated.
And despite their early successes with their next-gen cocktail, Immune Biosolutions’ Finzi added a note of caution:
“We shouldn’t underestimate the capacity of a coronavirus to mutate.”
Joint pain is a common lupus symptom, but the chronic condition can affect nearly every organ in the body. Image: Shutterstock (Shutterstock)
Scientists in Germany may have demonstrated a new way to treat and possibly even cure the chronic condition lupus. In a study out Thursday, the team describes how patients given a form of immunotherapy currently used to treat certain cancers have experienced a sustained remission of their symptoms, along with the autoantibodies that trigger the illness. More data will be needed to confirm the breakthrough potential of the treatment, however.
Lupus is a complex chronic disease, caused by a wayward immune system, that affects about 1.5 million Americans. There are several forms of lupus, some of which affect specific parts of the body, such as the skin. But the most common version is systemic lupus erythematosus (SLE), which can affect nearly every organ in the body. Symptoms of SLE often vary from person to person, and it may take years for someone to know that they have lupus. That said, a common trademark of the condition is chronic inflammation, which can manifest as joint pain, fever, and skin rashes.
Most cases of lupus are diagnosed between the ages of 15 and 44 and have no clear cause, though it’s suspected that a person’s genetics and environmental triggers like viral infection play a vital role. Once symptoms occur, people will tend to experience flare-ups of illness. These flare-ups can be lessened or managed with treatments, but there is currently no cure for lupus itself.
The underlying defect behind lupus are antibodies that attack the body’s tissues. These autoantibodies are produced by a subset of B cells, the immune system’s antibody-making machinery. There are current treatments for lupus that try to deplete the body’s supply of B cells to shut off these antibodies, but these drugs have had limited effectiveness to date. In recent years, backed by early animal data, some scientists have theorized that a form of immunotherapy known as CAR T cell therapy can succeed where these drugs have failed.
The basic concept of CAR T cell therapy is to take a person’s T cells—immune cells trained to attack a specific target, like a foreign germ—and modify them in the lab to recognize targets on a cell’s surface that they would normally have trouble finding, such as those on certain cancer cells. But according to study author Georg Schett, an immunologist at the University of Erlangen-Nuremberg in Germany, the same antigen that can be found on malignant leukemia and lymphoma B cells can also be found on the B cells that produce lupus autoantibodies. This antigen is known as CD19.
In their new research, published Thursday in Nature Medicine, Schett and his team infused five patients with treatment-resistant SLE with modified anti-CD19 T cells. And so far, all of them have experienced a remarkable recovery. Their symptoms have all improved, with none showing signs of lupus-related internal damage up to 17 months later and minimal side-effects from the therapy. Crucially, the patients’ autoantibodies have seemingly disappeared as well, perhaps for good, since the antibodies didn’t return once their B cells began to replenish after an average 100 days later. As a result, the patients have not needed further treatment of any kind.
“That is fundamentally different from any other treatment so far,” Schett told Gizmodo in an email.
These findings could herald a medical breakthrough for lupus. But for now, they’re still based on a very small sample size, and there remain many questions about the therapy’s effectiveness—including whether these patients are truly cured and whether this will be the case for others with lupus as well. Other research teams are studying CAR T cell therapy for lupus, though, so we’re certain to have more data soon. If this research is validated, then the therapy may not just dramatically change the outlook for lupus patients but for many people with similar autoimmune conditions—a possibility that Schett’s team is already working to study in the near future.
“Our patients will be followed for a longer time to see if they stay healthy without treatment. We want to know whether they are cured or not,” Schett said. “We will also start a basket study, which will include different autoimmune diseases (lupus, myositis and systemic sclerosis) in order to move this program forward.”
Since the rollout of mRNA COVID-19 vaccines, many researchers have speculated on the possibility of transmission of vaccine particles from the vaccinated to the unvaccinated, more commonly known as “vaccine shedding.”
Though these speculations are routinely fact-checked, anecdotal stories of unvaccinated people who become infected with COVID-19 or have experienced strange symptoms after contact with friends or family who were vaccinated have persisted.
Several doctors have also speculated about possible transmission as new findings in support of these ideas emerge.
A recent pre-print study has attracted media attention as the results of the study may be interpreted as suggestive of vaccine transmission via shedding.
Illustration of antibodies (y-shaped) responding to an infection with the new coronavirus SARS-CoV-2. (Getty Images)
New Pre-Print Study Implies Airborne Antibodies From Vaccine
A new pre-print study published by the University of Colorado concluded that antibodies can be transmitted through aerosols.
In the study, unvaccinated children living in either vaccinated or unvaccinated households were nasal swabbed for COVID-19 antibodies.
The authors, led by Dr. Ross Kedl, found that children living with vaccinated parents have higher concentration of COVID-19 antibodies in their swabs than children living in unvaccinated households.
Antibodies are immune markers, and each person’s collection of antibodies is a reflection of immunization and infection history. The presence of each antibody indicates that the person may have been exposed to a particular infection or vaccine the antibody fights against.
Therefore, a person is only supposed to display antibodies to COVID-19 if they have been infected or vaccinated. Yet, these children have not been vaccinated against nor infected with COVID-19. Why do they have antibodies?
The authors of the study reasoned that the vaccinated parents likely passed their antibodies to the children. They produced antibodies from the vaccine, these antibodies accumulated in the nasal cavities and became airborne. Their children then breathed the antibodies in, accumulating COVID-19 antibodies in their nasal cavities.
This is a plausible speculation as it is well documented that bodily fluids including breastmilk, saliva, tears, and sweat contain antibodies. Mothers are also recommended to breastfeed their babies, as it provides their babies with antibodies, protecting them from infection.
Still, though we know that antibodies can be present in bodily fluids, we do not know if antibodies can become airborne.
To support their speculation that antibodies may be airborne, the authors tested face masks from vaccinated individuals and found COVID-19 antibodies on the masks.
The authors argued that since everyone breathes into their masks, the COVID-19 antibodies found on the masks could be evidence that antibodies can be aerosolized, and therefore transmitted to others.
Though, the authors acknowledged that antibodies could have come off from saliva and sweat.
However, internal medicine practitioner and integrative and chelating specialist Dr. Ana Maria Mihalcea questioned the conclusion.
She told The Epoch Times that the study leaves a lot open to interpretation, and the same findings can also be used to support speculations of vaccine shedding.
“[The study] says that the antibodies are being transferred,” she said. “But could it be that the spike protein has been transferred [through contact through skin] and the child has mounted its own antibody response? I don’t think that that’s really clear.”
Photograph of Dr. Ana Maria Mihalcea. (Courtesy of Dr. Mihalcea)
What Do We Know About Transmission?
Vaccine shedding, dubbed as “transmission” by Dr. Sherri Tenpenny, has remained a controversial topic in the discourse on COVID-19 vaccines as there has yet to be any study that proves or shows conclusive proof of shedding.
One topic of debate is that vaccine shedding may not be the most accurate definition for what clinicians suspect are happening.
Vaccine shedding specifically refers to the spreading of virus and viral particles after vaccination. Viral shedding has been observed with vaccines for oral forms of polio vaccines, rotaviruses, adenoviruses, influenza, and many more.
Shedding only happens for vaccines containing live and attenuated viruses.
After vaccination, viruses can be detected in fecal samples of the vaccinated, and those who come into contact with them may be infected if the shed viral particles are infectious.
However, the mRNA Pfizer and Moderna COVID-19 injections do not use live coronaviruses, rather only the spike protein mRNA is shipped into the cells inside a lipid nanoparticle.
Therefore, they cannot shed viruses, as there is no virus.
J&J and AstraZeneca both use weakened live adenoviruses (not coronavirus) to transport spike protein DNA. However, these viruses have been edited so that they cannot replicate in our cells, therefore, we also should not be able to shed COVID-19 vaccine adenoviruses either.
What about spike proteins then? As mentioned above, there are no studies that provide conclusive proof of spike protein transmission, though health experts are unwilling to rule out the possibility.
Many doctors have spoken up about the possibility of transmission of the particles contained in the COVID-19 injections from vaccinated individuals into the unvaccinated, causing possible symptoms.
File photo of human blood samples on an automated testing line. (David Silverman/Getty Images)
Curious Clinical Findings
Though there has been no study that gives proof of transmission, many doctors have observed strange occurrences in unvaccinated individuals after spending time with people who are vaccinated.
“What I’ve seen with unvaccinated individuals who would come into the office with symptoms of things like headaches, feeling unwell, myalgia (meaning muscle aches), and a lot of times women who got in contact with vaccinated people develop hemorrhaging and menstrual irregularities, but very unusual in terms of large clotting and bleeding,” Dr. Mihalcea told The Epoch Times.
She shared a recent case of two unvaccinated menopausal women who started hemorrhaging after sitting together with a recently vaccinated individual for two hours in a car ride.
“The vaccinated person had just gotten their shot a week earlier, and the two unvaccinated women when they got out of the car after a two hour car ride, they both started bleeding.”
Mihalcea cited Pfizer clinical trials as another indication of possible vaccine transmission or shedding.
The Pfizer clinical trials (pdf) listed vaccine exposure during pregnancy (EDP) as an event that needed to be reported and monitored.
Though exposure could occur by participating in the study and getting vaccinated, or getting exposed through a vaccinated male partner through sexual contact, Mihalcea expressed concern at Pfizer’s listing of EDP through “environmental exposure.”
The Pfizer document said that examples of environmental exposure during pregnancy includes, “a female family member or healthcare provider reports that she is pregnant after having been exposed to the study intervention by inhalation or skin contact.”
This means that pregnant women may be exposed to the injection if breathing near or touching someone who was vaccinated.
EDP through environmental exposure would also be counted if, “a male family member or healthcare provider who has been exposed to the study intervention by inhalation or skin contact then exposes his female partner prior to or around the time of conception.”
This statement suggests that someone can be exposed to the vaccine through breathing or skin contact with someone who was vaccinated, and then pass it to someone else.
Findings from peer-reviewed research published in the Gazette of Medical Sciences also seem to be in support of vaccine transmission.
The study, which is based on a survey conducted by My Cycle Story, documented a spike in occurrences of decidual cast shedding and miscarriages in women after COVID-19 vaccines started rolling out.
One poignant testimony (pdf) in the study told of a woman of unknown vaccination status who experienced decidual cast shedding after her husband spent 20 minutes with people who were vaccinated.
Decidual cast shedding is a rare event. Around 40 cases have been documented in the medical literature, and it occurs when the thick mucus lining of the uterus sheds in nearly the exact shape of the inside of the uterus, creating a triangular cast.
This event is so rare that very few studies have been published about it, yet My Cycle Story reported 292 out of 6,092 women surveyed have experienced it following the rollout of COVID-19 vaccines. The study was also supplemented with testimonies from women who previously had successful pregnancies but began to suffer miscarriages after visiting friends and family who were vaccinated.
Though these cases may be a coincidence, Mihalcea’s own observations of unvaccinated patients developing various COVID-associated and strange conditions following contact with someone who was vaccinated made her suspicious that transmission was happening.
At the same time, other findings were also emerging that solidified Mihalcea’s suspicions.
A Canadian doctor, Dr. Charles Hoffe, announced in July 2021, that he found over 60 percent of his vaccinated patients had elevated D-dimer levels, and made his findings into a video.
D-dimer testing is often done to check for blood clots. Though elevated D-dimer levels are not conclusive of blood clots, they definitely indicate that possibility.
Mihalcea started doing her own D-dimer tests on unvaccinated patients who were concerned about vaccine transmission or showing conditions suggestive of possible transmission.
“I started seeing a huge amounts of [unvaccinated] people of all ages who had abnormal D-dimer testing, indicating the possibility for micro clotting,” Mihalcea said.
Mihalcea also published a video explaining elevated D-dimer levelsin her patients, suggesting possible transmission from vaccinated to unvaccinated individuals.
She told The Epoch Times that, since the vaccine rollout, she has treated many long COVID patients and cases of suspected transmission. She said that she has treated around 90 to 100 cases of suspected transmission, and brought their levels of D-dimers back down through her treatment regimen.
She has also since bought a microscope with which to analyze her patients’ blood through a prick test, by taking a prick of their blood and examining it under the microscope.
Blood analysis is normally done by pathologists, and many primary care physicians may choose to not analyze their patients’ blood, but Mihalcea, and many other doctors, have decided to investigate themselves.
Her treatment regime involved a series of supplements and pharmaceuticals, namely, ivermectin and hydroxychloroquine, both of which are effective antivirals for the COVID-19 virus. She also prescribes quercetin which reduces inflammation, glutathione has detox effects, blood thinners such as aspirin to prevent blood clotting, and vitamins to boost the immune system including vitamins D and C.
She said she later found vitamin C infusions, and chelating therapies, which remove heavy metals, also improved her patients’ symptoms and brought their D-dimer levels back to normal.
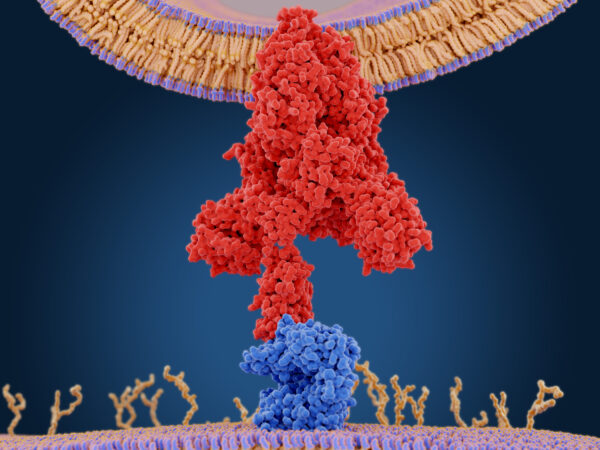
The coronavirus spike protein (red) mediates the virus entry into host cells. It binds to the angiotensin converting enzyme 2 (blue) and fuses viral and host membranes. By Juan Gaertner/Shutterstock
Doctors’ Speculations on What Is Happening
Clinicians do not know how and why unvaccinated people are developing these symptoms; however, many suspect it could be transmission of vaccine particles from the vaccinated to the unvaccinated.
Dr. Sherri Tenpenny said on the JD Rucker podcast that she and many doctors have come to the conclusion that the spike protein, made in human cells from the mRNA and adenovirus COVID-19 vaccines, are what is being transmitted from vaccinated to unvaccinated.
A study on cells in the laboratory has found that after exposure to spike protein DNA, cells derived from human embryonic kidney cells would make the spike proteins and then pack them into cellular sacs called exosomes.
Exosomes have been found in sweat and tears and have been previously studied as an option to impart immunity through skin contact.
Mihalcea said that exosomes could be transmitting spike proteins from infected cells since other studies have found that exosomes can be shed in sweat and tears, and this makes the possibility of transmission through skin contact and aerosols plausible.
Nonetheless, Mihalcea highlighted that since clinicians have no idea what is in the injection vials, if transmission is occurring, there also may be other things being transmitted apart from spike proteins.
Studies have long shown that the quality of vaccine vials can vary between batches.
The same applies to COVID-19 vaccines.
How Bad is My Batch, a website that compiles vaccine adverse event reports from Vaccine Adverse Event Reporting System (VAERS), has shown that the number of adverse effects can drastically vary between different batches of COVID-19 injections.
The website states that 5 percent of the Pfizer batches appear to have produced 90 percent of the Pfizer-associated adverse reactions, and that some batches are associated with 30 times the number of deaths and disabilities compared to other batches.
Mihalcea said that this variability reflects possible differences in injection content, and therefore every patient who reports vaccine transmission may respond differently.
“We cannot respond to this problem of shedding if every vial or every batch is not the same. There are certain batches that have very substantial side effects. That means that different batches don’t shed at all and other batches shed a lot.”
Recent peer-reviewed studies from Germany and Italy found that in mRNA-vaccinated people reporting post-vaccination symptoms, over 90 percent of the vaccinated had metal nanoparticles that resembled graphene oxide in their blood.
Vaccine manufacturers have assured that graphene is not in the COVID-19 vaccinations, and therefore the source of these nanoparticles is unknown.
Blood analyses by Dr. Phillipe Van Waldenberg have also found graphene oxide in the blood of both vaccinated and unvaccinated individuals.
Waldenberg first spotted “tube-like” graphene oxide particles in his vaccinated patients who were reporting symptoms of fatigue, dizziness, memory problems, and even paralysis, and late-onset heavy menstruation in menopausal women.
However, he later found these particles in unvaccinated individuals reporting paralysis symptoms as well.
Graphene oxide nanoparticles are used in biotechnology for cancer treatment and drug delivery. However, the material can be toxic to humans if inhaled, with varying levels of toxicity depending on its dosage, entry method, and pharmacokinetics.
Waldenberg reported his findings on Loving Life TV, speculating that transmission of graphene oxide is occurring between vaccinated and unvaccinated people. He said that one of his patients is an unvaccinated boy who reported paralysis in his limbs after his mother was vaccinated.
By Kudriavtsev Aleksei/Shutterstock
Should Unvaccinated Individuals Be Concerned?
If the things Mihalcea and many other doctors are saying are true, then the possibility of transmission poses significant health concerns for the unvaccinated.
Mihalcea recommended the unvaccinated to boost their immune systems through supplements. More importantly, however, she said that everyone should maintain a healthy mindset, including having no fear.
“When people are afraid, their immune system is adversely affected … If you’re depressed or you’re anxious, you actually shorten your telomeres (DNA which prevent aging) which means you’re aging much, much faster, including your immune system. So part of being healthy is also not being afraid.”
Social stress and anxiety have been associated with the shortening of telomeres, which increases aging, including aging of the immune system. Therefore, maintaining health mentally and emotionally is imperative for physical well-being.
To prevent transmission and its symptoms, Mihalcea advised unvaccinated people to boost their immune system by taking supplements such as vitamins C and D.
Nevertheless, Mihalcea said that the extent of transmission and the health symptoms have greatly varied. After treatment, some people’s D-dimers remained low even in contact with vaccinated people, and some people’s D-dimers went back up.
For the people who may be concerned about possible transmission or are experiencing suspected symptoms, “find physicians who are more open-minded,” said Mihalcea.
Some people’s primary care doctors who believe COVID vaccines cannot be the cause of their patients’ concerns may not be able to give suitable advice and support. Therefore Mihalecea advised people to find doctors “who are more open-minded and have a lot of information.”
By Iurii Motov/Shutterstock
Rebuttal and Controversy
Injection particle transmission, colloquially known as vaccine shedding, remains a controversial topic for COVID-19 injections.
Since there has been no study of nor precedent for transmission of mRNA and adenovirus DNA vaccinations, many doctors are waiting for more science to be published, discussing their clinical observation and piecing together findings from limited science.
Since many of these observations are anecdotal, and have not been through rigorous scientific reviewing, many of their statements and observations on vaccine transmission have been routinely fact-checked.
The public and doctors are still waiting for more research and discussion so that they can better understand these symptoms, and until more studies emerge, transmission between vaccinated and unvaccinated individuals will remain a theory that cannot be proven nor disproven.
Two antibodies that neutralize all known strains of COVID-19 – including Omicron – with up to 95% efficiency have been isolated by researchers. There is the possibility that these antibody treatments may make repeated booster shots for new variants unnecessary.
Tel Aviv University scientists have isolated two antibodies that neutralize all known strains of
Dr. Natalia Freund. Credit: Tel Aviv University
The current study is a continuation of a preliminary study that was conducted in October 2020, at the height of the COVID-19 crisis. At that time, Dr. Freund and her colleagues sequenced all the B immune system cells from the blood of people in Israel who had recovered from the original COVID strain. They isolated nine antibodies that the patients produced. The scientists have now found that some of these antibodies are exceptionally effective in neutralizing the new coronavirus variants, Delta and Omicron.
Dr. Freund: “In the previous study, we showed that the various antibodies that are formed in response to infection with the original virus are directed against different sites of the virus. The most effective antibodies were those that bound to the virus’s ‘spike’ protein, in the same place where the spike binds to the cellular receptor ACE2. Of course, we were not the only ones to isolate these antibodies, and the global health system made extensive use of them until the arrival of the different variants of the coronavirus, which in fact rendered most of those antibodies useless.
“In our view, targeted treatment with antibodies and their delivery to the body in high concentrations can serve as an effective substitute for repeated boosters, especially for at-risk populations and those with weakened immune systems.” — Dr. Natalia Freund
“In the current study, we proved that two other antibodies, TAU-1109 and TAU-2310, which bind the viral spike protein in a different area from the region where most of the antibodies were concentrated until now (and were, therefore, less effective in neutralizing the original strain) are actually very effective in neutralizing the Delta and Omicron variants. According to our findings, the effectiveness of the first antibody, TAU-1109, in neutralizing the Omicron strain is 92%, and in neutralizing the Delta strain, 90%. The second antibody, TAU-2310, neutralizes the Omicron variant with an efficacy of 84%, and the Delta variant with an efficacy of 97%.”
Dr. Freund believes that the surprising effectiveness of these antibodies might be related to the evolution of the virus.
“The infectivity of the virus increased with each variant because each time, it changed the amino
Israeli scientists say they have identified antibodies that are so powerful in neutralizing the coronavirus that they could eliminate the need for more vaccine boosters.
A research team at Tel Aviv University experimented with numerous antibodies and found that two in particular neutralize all known strains of the coronavirus, including Delta and Omicron, in a lab setting.
Antibody infusions are already used to treat some coronavirus patients, and microbiologist Dr. Natalia Freund, who directed the new study, said the antibodies she identified could be used to concoct a particularly potent infusion.
Based on their performance in lab conditions, the antibodies could provide the extra protection that today comes from booster shots, she said, adding that this could potentially make extra shots unnecessary among vaccinated people.
“COVID-19 infection can cause serious illness, and we know that providing antibodies in the first days following infection can stop the spread of the virus,” Freund said.
Sign up for the Tech Israel Daily and never miss Israel’s top tech stories
By signing up, you agree to the terms
“It is therefore possible that by using effective antibody treatment, we will not have to provide booster doses to the entire population every time there is a new variant,” she added.
According to Freund, on a technical level, the reason for the success of the two antibodies seems to be that they bind to a different part of the coronavirus spike protein than most others.
Illustrative image: a coronavirus ward at the Barzilai Medical Center, in Ashkelon, Israel, Thursday, Aug. 26, 2021. (AP Photo/Maya Alleruzzo)
Freund’s latest research, newly peer-reviewed and published in Communications Biology, comes from investigations that began in her lab in October 2020.
Working with doctoral students Michael Mor and Ruofan Lee, she sequenced all the B immune system cells from the blood of people who had recovered from the original COVID strain in Israel, and isolated nine antibodies that the patients produced.
Now, the top two antibodies have been tested against a range of variants, and performed well against all of them.
“According to our findings, the effectiveness of the first antibody, TAU-1109, in neutralizing the Omicron strain is 92 percent, and in neutralizing the Delta strain, 90%,” Freund said.
“The second antibody, TAU-2310, neutralizes the Omicron variant with an efficacy of 84%, and the Delta variant with an efficacy of 97%,” she added.
The antibodies are named TAU because they were identified at Tel Aviv University.
To ensure that her lab work was done correctly, Freund sent the antibodies to have their effectiveness against live viruses checked in laboratory cultures at the University of California San Diego, and for further testing at Bar-Ilan University’s medicine faculty in the Galilee. These studies corroborated her findings.
Natalia Freund of Tel Aviv University (courtesy of Tel Aviv University)
Freund said that antibodies clearly give strong protection, as they prevent infection straight after recovery — but then they wane, and immunity reduces. In her view, this makes it logical to invest in artificially boosting antibodies, and she hopes to do exactly this with the antibodies she identified.
“For reasons we still don’t yet fully understand, the level of antibodies against COVID-19 declines significantly after three months,” she explained. “This is why we see people getting infected again and again, even after being vaccinated three times.
“COVID-19 infection can cause serious illness, and we know that providing antibodies in the first days following infection can stop the spread of the virus. It is therefore possible that by using effective antibody treatment, we will not have to provide booster doses to the entire population every time there is a new variant.”
You’re a dedicated reader
We’re really pleased that you’ve read X Times of Israel articles in the past month.
That’s why we started the Times of Israel ten years ago – to provide discerning readers like you with must-read coverage of Israel and the Jewish world.
So now we have a request. Unlike other news outlets, we haven’t put up a paywall. But as the journalism we do is costly, we invite readers for whom The Times of Israel has become important to help support our work by joining The Times of Israel Community.
For as little as $6 a month you can help support our quality journalism while enjoying The Times of Israel AD-FREE, as well as accessing exclusive content available only to Times of Israel Community members.
Thank you, David Horovitz, Founding Editor of The Times of Israel
Aside from the vaccine, one of the biggest reasons we’ve seen a drop in COVID deaths since the start of the pandemic is because of the development of effective treatments. Doctors and nurses are better equipped to help patients who come in with a serious case of the virus, shortening hospital stays and alleviating pressure on a strained medical system. And, as time passes, better and more effective treatments are being discovered—and sometimes in very surprising places.
That’s the case with some new research led by a team at Mount Sinai Hospital who discovered a strong “super-immunity” particle in llamas’ blood. Yes, you read that correctly: llamas’ blood. The same creatures known for chewing cud, spitting at tourists, and being voiced by David Spade.
In a study published today in the journal Cell Reports, the researchers found evidence that tiny immune molecules in llamas known as nanobodies could help develop an inhalable antiviral drug for COVID patients to serve as a fast-acting treatment to the pandemic. Moreover, the research suggests that it protects against every COVID variant—meaning we may have a future-proof treatment that will remain effective as the virus evolves.
“We learned that the tiny size of these nanobodies gives them a crucial advantage against a rapidly mutating virus,” Ian Wilson, a professor of structural biology at Scripps Research in La Jolla, California and co-author of the study, said in a press release. “Specifically, it allows them to penetrate more of the recesses, nooks, and crannies of the virus surface, and thus bind to multiple regions to prevent the virus from escaping and mutating.”
Creatures specifically in the biological family Camelidae including camels, alpacas, and llamas are capable of producing tiny antibodies that are about a tenth the size of a normal one. Despite their size, the antibodies are very hardy and can glom onto disease-causing intruders like the coronavirus very well. The researchers were able to hack the antibodies and link them together, ensuring that they’re even more effective against viruses.
“Because of their small size and broad neutralizing activities, these camelid nanobodies are likely to be effective against future variants and outbreaks of SARS-like viruses,” Yi Shi, associate professor of pharmacological sciences at Mount Sinai and lead author of the study, said in the release.
Shi added that the antibodies are also capable of protecting “both the upper and lower respiratory tracts against infection,” indicating they could be an effective drug when paired with vaccine and current antibody treatments.
This study builds off previous research into the awesome, super-immunity powers of llamas’ blood that actually predates the pandemic. With the urgency of the pandemic, though, it makes sense that researchers would want to revisit our wooly, mountain-climbing friend.
However, it’d behoove everyone to keep in mind that this is still in fairly early stages. Much more research needs to be done in order to refine and develop an actual treatment. And if the whole horse dewormer fiasco has taught us anything, it’s that we should avoid jumping to knee jerk conclusions before the research has been done.
In other words, for the love of everything holy, don’t go out and start slaughtering llamas and drinking their blood. That won’t help you. It’ll do the opposite of helping you. In fact, you might end up being cursed a la “The Emperor’s New Groove” and become a llama yourself.
However, Covid-19 vaccination is still expected to provide substantial protection against severe disease, and vaccine makers are working on updated shots that might elicit a stronger immune response against the variants.
“We observed 3-fold reductions of neutralizing antibody titers induced by vaccination and infection against BA4 and BA5 compared with BA1 and BA2, which are already substantially lower than the original COVID-19 variants,” Dr. Dan Barouch, an author of the paper and director of the Center for Virology and Vaccine Research at Beth Israel Deaconess Medical Center in Boston, wrote in an email to CNN.
“Our data suggest that these new Omicron subvariants will likely be able to lead to surges of infections in populations with high levels of vaccine immunity as well as natural BA1 and BA2 immunity,” Barouch wrote. “However, it is likely that vaccine immunity will still provide substantial protection against severe disease with BA4 and BA5.”
The newly published findings echo separate research by scientists at Columbia University.
They recently found that the BA.4 and BA.5 viruses were more likely to escape antibodies from the blood of fully vaccinated and boosted adults compared with other Omicron subvariants, raising the risk of vaccine-breakthrough Covid-19 infections.
The authors of that separate study say their results point to a higher risk for reinfection, even in people who have some prior immunity against the virus. The US Centers for Disease Control and Prevention estimates 94.7% of the US population ages 16 and older have antibodies against the coronavirus that causes Covid-19 through vaccination, infection, or both.
BA.4 and BA.5 caused an estimated 35% of new Covid-19 infections in the United States last week, up from 29% the week before, according to data shared by the US Centers for Disease Control and Prevention on Tuesday.
BA.4 and BA.5 are the fastest spreading variants reported to date, and they are expected to dominate Covid-19 transmission in the United States, United Kingdom and the rest of Europe within the next few weeks, according to the European Centre for Disease Prevention and Control.
‘COVID-19 still has the capacity to mutate further’
In the New England Journal of Medicine paper, among 27 research participants who had been vaccinated and boosted with the Pfizer/BioNTech coronavirus vaccine, the researchers found that two weeks after the booster dose, levels of neutralizing antibodies against Omicron subvariants were much lower than the response against the original coronavirus.
The neutralizing antibody levels were lower by a factor of 6.4 against BA.1; by a factor of 7 against BA.2; by a factor of 14.1 against BA.2.12.1 and by a factor of 21 against BA.4 or BA.5, the researchers described.
Among 27 participants who had previously been infected with the BA.1 or BA.2 subvariants a median of 29 days earlier, the researchers found similar results.
In those with previous infection — most of whom also had been vaccinated — the researchers described neutralizing antibody levels that were lower by a factor of 6.4 against BA.1; by a factor of 5.8 against BA.2; by a factor of 9.6 against BA.2.12.1 and by a factor of 18.7 against BA.4 or BA.5.
More research is needed to determine what exactly the neutralizing antibody levels mean for vaccine effectiveness and whether similar findings would emerge among a larger group of participants.
“Our data suggest that COVID-19 still has the capacity to mutate further, resulting in increased transmissibility and increased antibody escape,” Barouch wrote in the email. “As pandemic restrictions are lifted, it is important that we remain vigilant and keep studying new variants and subvariants as they emerge.”
A separate study, published in the journal Nature last week, found that Omicron may evolve mutations to evade the immunity elicited by having a previous BA.1 infection, which suggests that vaccine boosters based on BA.1 may not achieve broad-spectrum protection against new Omicron subvariants like BA.4 and BA.5.
As for what all this means in the real world, Dr. Wesley Long, an experimental pathologist at Houston Methodist Hospital, told CNN that people should be aware that they could get sick again, even if they’ve had Covid-19 before.
“I think I’m a little bit worried about people who’ve had it maybe recently having a false sense of security with BA.4 and BA.5 on the increase, because we have seen some cases of reinfection and I have seen some cases of reinfection with people who had a BA.2 variant in the last few months,” he said.
Some vaccine makers have been developing variant-specific vaccines to improve the antibody responses against coronavirus variants and subvariants of concern.
“Reinfections are going to be pretty inevitable until we have vaccines or widespread mandates that are going to prevent cases rising again. But the good news is that we are in, I think, a much better spot than we were without the vaccines,” said Pavitra Roychoudhury, an acting instructor at the University of Washington’s Department of Laboratory Medicine and Pathology, who was not involved in the New England Journal of Medicine paper.
“There’s so much of this virus out there that it seems inevitable,” she said about Covid-19 infections. “Hopefully the protections that we have in place are going to lead to mostly mild infection.”
Efforts underway to update Covid-19 vaccines
Moderna’s bivalent Covid-19 vaccine booster, named mRNA-1273.214, elicited a “potent” immune responses against the Omicron subvariants BA.4 and BA.5, the company said Wednesday.
This bivalent booster vaccine candidate contains components of both Moderna’s original Covid-19 vaccine and a vaccine that targets the Omicron variant. The company said it is working to complete regulatory submissions in the coming weeks requesting to update the composition of its booster vaccine to be mRNA-1273.214.
“In the face of SARS-CoV-2’s continued evolution, we are very encouraged that mRNA-1273.214, our lead booster candidate for the fall, has shown high neutralizing titers against the BA.4 and BA.5 subvariants, which represent an emergent threat to global public health,” Stéphane Bancel, chief executive officer of Moderna, said in Wednesday’s announcement. SARS-CoV-2 is the coronavirus that causes Covid-19.
“We will submit these data to regulators urgently and are preparing to supply our next generation bivalent booster starting in August, ahead of a potential rise in SARS-CoV-2 infections due to Omicron subvariants in the early fall,” Bancel said.
The US Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee is meeting next week to discuss the composition of Covid-19 vaccines that could be used as boosters this fall.
The data that Moderna released Wednesday, which has not been published in a peer-reviewed journal, showed that one month after a 50-microgram dose of the mRNA-1273.214 vaccine was administered in people who had been vaccinated and boosted, the vaccine elicited “potent” neutralizing antibody responses against BA.4 and BA.5, boosting levels 5.4-fold in all participants regardless of whether they had a prior Covid-19 infection and by 6.3-fold in the subset of those with no history of prior infection. These levels of neutralizing antibodies were about 3-fold lower than previously reported neutralizing levels against BA.1, Moderna said.
These findings add to the data that Moderna previously released earlier this month, showing that the 50-microgram dose of the bivalent booster generated a stronger antibody response against Omicron than the original Moderna vaccine.
Moderna’s data suggest that “the bivalent booster might confer greater protection against the BA.4 and BA.5 omicron strains than readministering the original vaccine to increase protection across the population. Although the information is based on antibody levels, the companies comment that similar levels of antibody protected against clinical illness caused by other strains is the first suggestion of an emerging ‘immune correlate’ of protection, although it is hoped that this ongoing study is also assessing rates of clinical illness as well as antibody responses,” Penny Ward, an independent pharmaceutical physician and visiting professor in pharmaceutical medicine at King’s College London, said in a statement released by the UK-based Science Media Centre on Wednesday. She was not involved in Moderna’s work.
“It has been reported previously that the bivalent vaccine is well tolerated with temporary ‘reactogenic’ effects similar to those following the univalent booster injection so we can anticipate that this new mixed vaccine should be well tolerated,” Ward said in part. “As we head towards the autumn with omicron variants dominating the covid infection landscape, it certainly makes sense to consider use of this new bivalent vaccine, if available.”
The uptick in COVID cases these days is driven a lot of different factors—in great part the emergence of highly contagious variants like omicron and a drop in masking and social distancing rules, but also an overall waning in immunity for those who are vaccinated, which is no surprise. Antibodies, whether prompted by infection or vaccination, naturally taper off over a couple of months (or quicker depending on a person’s age and health). As COVID threatens to be a permanent house guest, scientists are starting to develop new ways to assess immune status quickly and easily.
Working toward that goal, researchers in Hong Kong have developed a device that allows someone to directly see their antibody levels following vaccination. The device, detailed in a new paper published Friday in the journal Science Advances, is on par with conventional coronavirus antibody testing platforms. It could be used as a better way to conduct mass screening for COVID immunity, to monitor someone’s immune status after the jab, or to even tailor vaccine dosing to an individual’s immune needs.
The most accurate antibody testing available right now requires blood samples that are analyzed in a lab. There are more convenient, at-home options that test your spit or nasal secretions. The problem with these more accessible kits is that they can only give you a yes or no and don’t factor in the level of antibody coursing in your body, Ting-Hsuan Chen, a biomedical engineer at the City University of Hong Kong and the study’s lead researcher, told The Daily Beast.
The new device, which can fit in the palm of your hand, consists of a small clear chip carrying two types of microparticles, tiny channels, and a little window to see the final result. One microparticle is magnetic and coated in the virus’s spike protein. The other is made of a compound called polystyrene and is studded with antibodies that attract anti-COVID antibodies, which typically target the spike protein.
Users just need to provide a few small drops of blood plasma from a finger prick. If COVID antibodies are present, they will attach to the polystyrene microparticles, which in turn will attach to the magnetic microparticles. The joined microparticles are magnetically separated from the single ones and collect in the little viewing window, called a particle dam. A little bar etched next to the side of the dam corresponds to the concentration of antibodies present as nanograms per milliliter.
Chen and his team tested out the device in 91 people who had received their second vaccine dose a few weeks prior. The team found that antibody levels were the highest for those who received an mRNA vaccine. But for everyone, antibody levels dropped off substantially after 45 days. These results were comparable to antibody tests done in a lab and were even better at detecting low levels of antibodies compared to at-home detection kits, which barely registered a positive.
It’s important to note that even though your antibody levels naturally decline, that doesn’t mean you outright lose the ability to make antibodies. After vaccination or infection, your body creates a memory of the antigen it learns to target and if it ever reappears, the immune system can quickly launch an attack.
However, Chen said it still takes time for your body to reactivate that memory and remake the necessary antibodies. In this situation, the new testing device could come in handy: During an outbreak, health agencies, clinicians, or people themselves could monitor antibody levels and see who among those previously vaccinated aren’t mounting a strong enough response and may need a booster shot. This could lead to more personalized vaccine dosing whether based on age—older people tend to not develop as robust immune responses after vaccination—or health status, such as if you’re immunocompromised.
Chen and his team are still working on making the device more accessible, such as making it capable of detecting antibodies in samples like spit or nasal secretions, which would make the device possible for home use.
“Our vision is to provide a device as simple as a rapid test but also provides as good accuracy as [conventional antibody testing],” Chen said. “I usually make an analogy to a mercury thermometer. It’s a device you can see and take temperature precisely without any equipment and that everyone can use. We hope our device can be like that, simple to use and everyone can read without any ambiguity to get the results they need.”
In what seemed like an instant, COVID-19 became an inevitable aspect of everyday life more than two years ago — with no signs to suggest that we’ll ever see otherwise again.
As we look at our lives ahead with waves of new variants and “stealth” sub-variants, and seasonal vaccine boosters to match, it begs the question: Should we fear reinfection?
Doctors have recently confirmed that those infected with an earlier Omicron variant, which first appeared and spread rapidly last summer, can indeed test positive again for the new sub-variant.
Last week, as the latest strain — BA.2 or BA2.12.1 — made its presence known in New York City and clusters throughout the Northeast and Midwest, the US crossed a grim milestone: 1 million COVID deaths. Globally, we’ve lost more than 6 million.
The Post spoke to NYU Langone Health infectious diseases expert Dr. Michael Phillips about what we can expect from life with COVID as we know it.
Can you get infected with COVID twice — and who’s at risk?
There is no such thing as perfect immunity from COVID. Regardless of severity or immunization, someone who tests positive for the virus can become infected again at some point.
“Our hospitalizations have crept up over the past several weeks, particularly with this newer variant of Omicron,” Dr. Phillips told The Post. “But thankfully, the vast majority of people [who] get the infection tend to recover without too much problems.”
But there’s more at stake for some. People who have not received two doses of the mRNA vaccine, as well as those with weakened immune systems due to age, medications, preexisting illness or other clinical factors, such as poor physical fitness, are at a higher risk of reinfection and becoming severely sick with COVID-19.
Phillips warns against us “develop[ing] a laissez faire attitude about it.” While some relatively young, healthy and vaccinated individuals may become reinfected with only a mild case, the person they pass it to — potentially, someone with a weakened immune system due to age, medications, preexisting illness or other clinical factors, such as poor physical fitness — may not fare so well.
Omicron is “very, very different from prior waves of Delta,” Phillips added. “I think it shifted our game plan for sure.” Now more than ever the focus of prevention efforts is on protecting the ones at a greater risk of severe illness — and protecting yourself from COVID reinfection means also “protect[ing] the vulnerable.”
Can you be reinfected with the same COVID variant?
It’s certainly possible, particularly in those who are not vaccinated. Unlike earlier variants, Omicron has rapidly evolved into several sub-types, prompting simultaneous localized outbreaks. Meanwhile, there’s no telling how many positive cases of COVID-19 go unreported, whether due to lack of testing or absence symptoms warranting alarm. So whether to fear reinfection with the same niche strain may not be a pragmatic question to ask — because, by the time it’s answered, a new strain may already be here.
“There are so many of these other variants within that big family of coronaviruses, and we’re typically infected with three to four a year,” Phillips explained, most of which present as a mild cold.
Ideally, SARS-CoV-2 could fade into coronavirus obscurity like many of the others — but we aren’t there yet, and it’s too soon to say whether that’s a feasible outlook. “It’s still severe enough that that we have to be pretty mindful about,” said Phillips. “We just don’t know enough about future variants for us to take our guard down yet.”
New York City residents are currently on “high alert” as of Wednesday, May 18, 2022.New York City Department of Health and Mental Hygiene
How long after getting COVID can you be reinfected?
This is another complicated question — especially for sufferers of long COVID, who appear to harbor low, even undetectable levels of the virus for weeks and months. For mild to moderate cases, people who test positive for COVID can expect their infection to clear within five to 10 days after their symptoms arose, or since their confirmed test result.
Nascent research suggests that the average immune system can fend off COVID reinfection for three to five months after the previous bout. That’s why, according to the Centers for Disease Control and Prevention, people who had a confirmed infection within the previous 90 days are not expected to quarantine after coming in contact with another infected individual.
But all bets are off about six months later, when antibodies are known to start waning — regardless of vaccination.
How long do COVID antibodies last?
Experts don’t know exactly. While those who survive COVID appear to be largely protected from repeat or severe illness for up to five months after the previous infection, there isn’t enough data available yet to be certain how long those COVID-specific antibodies linger, or even to confirm that the presence of antibodies guarantees immunity, according to the Food and Drug Administration.
Immune system B cells give rise to COVID-specific antibodies, designed to attack the virus on sight, before it can penetrate tissue cells and reproduce. They begin to form within the first few days infection or vaccination, and continue to build for several weeks until they peak at around three months thereafter — when your COVID defenses are at their strongest.
The good news is that waning antibodies doesn’t mean we’re totally defenseless, as some B cells will remember the steps it previously took to create COVID antibodies during re-invasion. (Boosters, furthermore, help our immune system remember how to fight.) Meanwhile, our killer T-cells, the immune system’s backup line of defense, may not be so good at preventing the virus from entering the body, but they can spot an infected host cell — and destroy it before it multiplies to another cell. And while they’re more difficult to track, they do appear to be more faithful than fleeting antibodies.
“Those appear to stay much more robust,” said Phillips, adding, that “the T-cell response is probably more important for response to viral infections” in the long run.
Are COVID vaccines still effective?
“We don’t have to be paranoid about the emergence of a new strain … but we have to be thoughtful and ready for that.”
Dr. Michael Phillips, NYU Langone Health
Vaccines remain the best way to build up antibodies, the body’s primary line of defense against severe COVID-19 illness. While allowing oneself to become infected can also give rise to antibodies, it’s not worth the risk.
“I’m strongly pro vaccine, because of the problems that happen when you don’t get it,” said Phillips, who hinted at alternative forms of vaccination technology on the horizon as well.
Regardless of type, antibodies are known to wane after about six months since last infection or booster, making reinfection more likely to occur.
How often can you get a COVID booster?
For those on the two-dose vaccine regimen, a second round should be completed about six weeks after the first. However, it’s been well over a year since the vaccine was introduced, which means many patients completed those two rounds back in 2021.
Doctors expect that annually, even seasonally redesigned boosters against COVID-19 could become the norm — kind of like influenza, only different, and more troubling: One flu season sees just one or two major strains globally, allowing researchers time to prepare vaccines. “It’s not this, sort of, constant changing during a ‘season,’ ” said Phillips, like COVID-19 has done.
Currently, only those who have a weakened immune system and people age 50 or older who got their first booster four months ago are being recommended for a second booster by the CDC — which is, altogether, a good sign.
Said Phillips, “We don’t have to be paranoid about the emergence of a new strain … but we have to be thoughtful and ready for that.”